Download
1 / 1
10 likes | 98 Views
5 th European Congress For Integrative Medicine - 21-22 September 2012, Firenze Reactive arthritis, immunomediate pathogenesis and Homeopathic therapy S Cavallo 1,2 , G Marinelli 1,2 , G De Paolis 1,2 , M Marsano 1,2 , A Di Francesco 1 , M Mancini 1,2,3

E N D
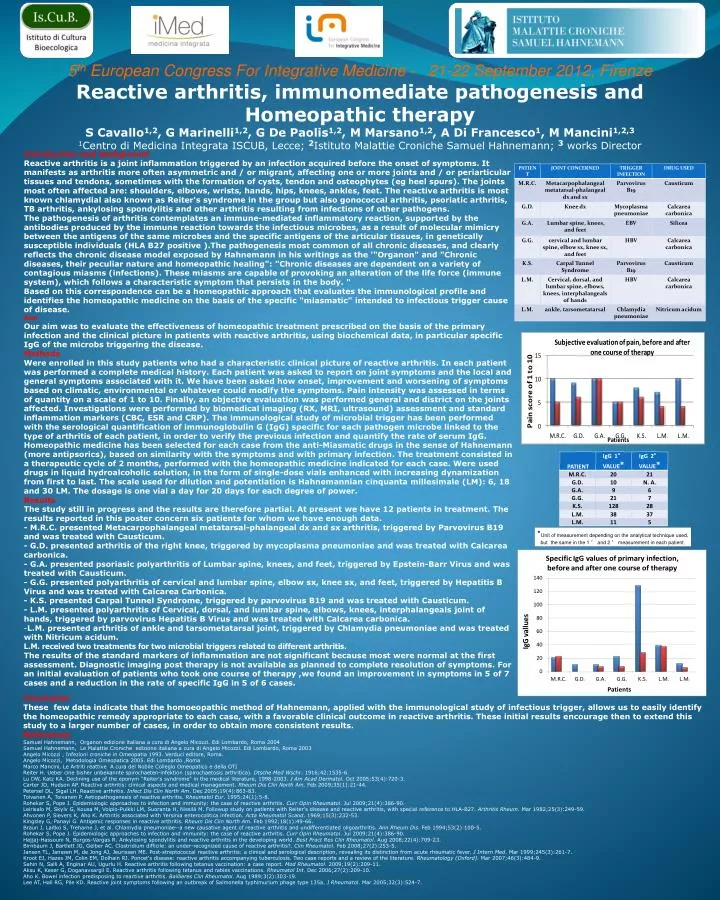
5th European Congress For Integrative Medicine - 21-22 September 2012, Firenze Reactive arthritis, immunomediate pathogenesis and Homeopathic therapy S Cavallo1,2, G Marinelli1,2, G De Paolis1,2, M Marsano1,2, A Di Francesco1, M Mancini1,2,3 1Centro di Medicina Integrata ISCUB, Lecce; 2Istituto Malattie Croniche Samuel Hahnemann; 3 works Director • Introduction and background • Reactive arthritis is a joint inflammation triggered by an infection acquired before the onset of symptoms. It manifests as arthritis more often asymmetric and / or migrant, affecting one or more joints and / or periarticular tissues and tendons, sometimes with the formation of cysts, tendon and osteophytes (eg heel spurs). The joints most often affected are: shoulders, elbows, wrists, hands, hips, knees, ankles, feet. The reactive arthritis is most known chlamydial also known as Reiter's syndrome in the group but also gonococcal arthritis, psoriatic arthritis, TB arthritis, ankylosing spondylitis and other arthritis resulting from infections of other pathogens. The pathogenesis of arthritis contemplates an immune-mediated inflammatory reaction, supported by the antibodies produced by the immune reaction towards the infectious microbes, as a result of molecular mimicry between the antigens of the same microbes and the specific antigens of the articular tissues, in genetically susceptible individuals (HLA B27 positive ).The pathogenesis most common of all chronic diseases, and clearly reflects the chronic disease model exposed by Hahnemann in his writings as the '"Organon" and "Chronic diseases, their peculiar nature and homeopathic healing": "Chronic diseases are dependent on a variety of contagious miasms (infections). These miasms are capable of provoking an alteration of the life force (immune system), which follows a characteristic symptom that persists in the body. " Based on this correspondence can be a homeopathic approach that evaluates the immunological profile and identifies the homeopathic medicine on the basis of the specific "miasmatic" intended to infectious trigger cause of disease. Aim • Our aim was to evaluate the effectiveness of homeopathic treatment prescribed on the basis of the primary infection and the clinical picture in patients with reactive arthritis, using biochemical data, in particular specific IgG of the microbs triggering the disease. • Methods • Were enrolled in this study patients who had a characteristic clinical picture of reactive arthritis. In each patient was performed a complete medical history. Each patient was asked to report on joint symptoms and the local and general symptoms associated with it. We have been asked how onset, improvement and worsening of symptoms based on climatic, environmental or whatever could modify the symptoms. Pain intensity was assessed in terms of quantity on a scale of 1 to 10. Finally, an objective evaluation was performed general and district on the joints affected. Investigations were performed by biomedical imaging (RX, MRI, ultrasound) assessment and standard inflammation markers (CBC, ESR and CRP). The immunological study of microbial trigger has been performed with the serological quantification of immunoglobulin G (IgG) specific for each pathogen microbe linked to the type of arthritis of each patient, in order to verify the previous infection and quantify the rate of serum IgG. Homeopathic medicine has been selected for each case from the anti-Miasmatic drugs in the sense of Hahnemann (more antipsorics), based on similarity with the symptoms and with primary infection. The treatment consisted in a therapeutic cycle of 2 months, performed with the homeopathic medicine indicated for each case. Were used drugs in liquid hydroalcoholic solution, in the form of single-dose vials enhanced with increasing dynamization from first to last. The scale used for dilution and potentiation is Hahnemannian cinquanta millesimale (LM): 6, 18 and 30 LM. The dosage is one vial a day for 20 days for each degree of power. • Results • The study still in progress and the results are therefore partial. At present we have 12 patients in treatment. The results reported in this poster concern six patients for whom we have enough data. • - M.R.C. presented Metacarpophalangeal metatarsal-phalangeal dx and sx arthritis, triggered by Parvovirus B19 and was treated with Causticum. • - G.D. presented arthritis of the right knee, triggered by mycoplasma pneumoniae and was treated with Calcarea carbonica. • - G.A. presented psoriasic polyarthritis of Lumbar spine, knees, and feet, triggered by Epstein-Barr Virus and was treated with Causticum. • - G.G. presented polyarthritis of cervical and lumbar spine, elbow sx, knee sx, and feet, triggered by Hepatitis B Virus and was treated with Calcarea Carbonica. • - K.S. presented Carpal Tunnel Syndrome, triggered by parvovirus B19 and was treated with Causticum. • - L.M. presented polyarthritis of Cervical, dorsal, and lumbar spine, elbows, knees, interphalangeals joint of hands, triggered by parvovirus Hepatitis B Virus and was treated with Calcarea carbonica. • L.M. presented arthritis of ankle and tarsometatarsal joint, triggered by Chlamydia pneumoniae and was treated with Nitricum acidum. • L.M. received two treatments for two microbial triggers related to different arthritis. • The results of the standard markers of inflammation are not significant because most were normal at the first assessment. Diagnostic imaging post therapy is not available as planned to complete resolution of symptoms. For an initial evaluation of patients who took one course of therapy ,we found an improvement in symptoms in 5 of 7 cases and a reduction in the rate of specific IgG in 5 of 6 cases. *Unit of measurement depending on the analytical technique used, but the same in the 1 ° and 2 ° measurement in each patient. Conclusion These few data indicate that the homoeopathic method of Hahnemann, applied with the immunological study of infectious trigger, allows us to easily identify the homeopathic remedy appropriate to each case, with a favorable clinical outcome in reactive arthritis. These initial results encourage then to extend this study to a larger number of cases, in order to obtain more consistent results. References Samuel Hahnemann, Organon edizione italiana a cura di Angelo Micozzi. Edi Lombardo, Roma 2004 Samuel Hahnemann, Le Malattie Croniche edizione italiana a cura di Angelo Micozzi. Edi Lombardo, Roma 2003 Angelo Micozzi , Infezioni croniche in Omeopatia 1993. Verduci editore, Roma. Angelo Micozzi, Metodologia Omeopatica 2005. Edi Lombardo ,Roma Marco Mancini, Le Artriti reattive A cura del Nobile Collegio Omeopatico e della OTI Reiter H. Ueber cine bisher unbekannte spirochaeten-infektion (spirochaetosis arthritica). Dtsche Med Wschr. 1916;42:1535-6. Lu DW, Katz KA. Declining use of the eponym "Reiter's syndrome" in the medical literature, 1998-2003. J Am Acad Dermatol. Oct 2005;53(4):720-3. Carter JD, Hudson AP. Reactive arthritis: clinical aspects and medical management. Rheum Dis Clin North Am. Feb 2009;35(1):21-44. Petersel DL, Sigal LH. Reactive arthritis. Infect Dis Clin North Am. Dec 2005;19(4):863-83. Toivanen A, Toivanen P. Aetiopathogenesis of reactive arthritis. Rheumatol Eur. 1995;24(1):5-8. Rohekar S, Pope J. Epidemiologic approaches to infection and immunity: the case of reactive arthritis. Curr Opin Rheumatol. Jul 2009;21(4):386-90. Leirisalo M, Skylv G, Kousa M, Voipio-Pulkki LM, Suoranta H, Nissilä M. Followup study on patients with Reiter's disease and reactive arthritis, with special reference to HLA-B27. Arthritis Rheum. Mar 1982;25(3):249-59. Ahvonen P, Sievers K, Aho K. Arthritis associated with Yersinia enterocolitica infection. Acta Rheumatol Scand. 1969;15(3):232-53. Kingsley G, Panayi G. Antigenic responses in reactive arthritis. Rheum Dis Clin North Am. Feb 1992;18(1):49-66. Braun J, Laitko S, Treharne J, et al. Chlamydia pneumoniae--a new causative agent of reactive arthritis and undifferentiated oligoarthritis. Ann Rheum Dis. Feb 1994;53(2):100-5. Rohekar S, Pope J. Epidemiologic approaches to infection and immunity: the case of reactive arthritis. Curr Opin Rheumatol. Jul 2009;21(4):386-90. Hajjaj-Hassouni N, Burgos-Vargas R. Ankylosing spondylitis and reactive arthritis in the developing world. Best Pract Res Clin Rheumatol. Aug 2008;22(4):709-23. Birnbaum J, Bartlett JG, Gelber AC. Clostridium difficile: an under-recognized cause of reactive arthritis?. Clin Rheumatol. Feb 2008;27(2):253-5. Jansen TL, Janssen M, de Jong AJ, Jeurissen ME. Post-streptococcal reactive arthritis: a clinical and serological description, revealing its distinction from acute rheumatic fever. J Intern Med. Mar 1999;245(3):261-7. Kroot EJ, Hazes JM, Colin EM, Dolhain RJ. Poncet's disease: reactive arthritis accompanying tuberculosis. Two case reports and a review of the literature. Rheumatology (Oxford). Mar 2007;46(3):484-9. Sahin N, Salli A, Enginar AU, Ugurlu H. Reactive arthritis following tetanus vaccination: a case report. Mod Rheumatol. 2009;19(2):209-11. Aksu K, Keser G, Doganavsargil E. Reactive arthritis following tetanus and rabies vaccinations. Rheumatol Int. Dec 2006;27(2):209-10. Aho K. Bowel infection predisposing to reactive arthritis. Baillieres Clin Rheumatol. Aug 1989;3(2):303-19. Lee AT, Hall RG, Pile KD. Reactive joint symptoms following an outbreak of Salmonella typhimurium phage type 135a. J Rheumatol. Mar 2005;32(3):524-7.