Download
1 / 20
200 likes | 336 Views
Double blinded placebo controlled crossover study of High Frequency SCS. C. Perruchoud , E. Buchser , A Durrer , B. Rutschmann , M. Rosato 1,2 , N. Bovet , A . Gulve 3 , M Brookes 3 , G. Madzinga 3 A. Batterham 4 and S . Eldabe 3.

E N D
Double blinded placebo controlled crossover study of High Frequency SCS C. Perruchoud, E. Buchser, A Durrer, B. Rutschmann, M. Rosato1,2, N. Bovet, A. Gulve3, M Brookes3, G. Madzinga3 A. Batterham4 and S . Eldabe3 1.Dept of Anaesthesiology and Pain Management Centre for Neuromodulation, Morges. Switzerland 2.Dept of Anaesthesiology and Pain Management University Hospital Center and University of Lausanne Switzerland 3. Dept of Anaesthesiology and Pain Management The James Cook University Hospital Middlesbrough UK 4. University of Teesside Middlesbrough UK
Disclosure • Medtronic funded the study and provided the technical support for IPG programming. • No member of Medtronic personnel contributed to the study design, data collection or data analysis. • The study was sponsored by the author’s institutions • E. Buchser, S. Eldabe and C. Perruchoud are Medtronic Consultants
Background • Double blinded controlled studies have not been feasible in SCS • In a randomised placebo controlled trial of 12 RA patients Eddicks showed Sub-threshold stimulation (SS) to have an analgesic effect1 • High Frequency (HF) stimulation and Burst stimulation produce analgesia without paraesthesias2,3 • In this study we aim to compare HF stimulation and Sham Stimulation in a double blind crossover design Eddicks, S., et al., Thoracic spinal cord stimulation improves functional status and relieves symptoms in patients with refractory angina pectoris: the first placebo-controlled randomised study. Heart, 2007. 93(5): p. 585-90. De Ridder, D., et al., Burst spinal cord stimulation: toward paresthesia-free pain suppression. Neurosurgery, 2010. 66(5): p. 986-90. Smet I, Van Buyten JP and Alkaisy A. Successful treatment of low back pain with a novel neurostimulation device. Proceeds of the North American Neuromodulation Society Meeting 2011 Las Vegas
Patients and Methods • 40 Patients with existing SCS systems (stable pain relief) implanted for low back and or leg pain enrolled at Morges Switzerland and Middlesbrough UK. • Patients Implanted with Restore Advanced/ Ultra/ Sensor and Prime Advanced. • A special study programmer allowed any of the IPGs to deliver the following settings • Frequency of 5'000 Hz continuous stimulation • Pulse width 60 μsec • Amplitude increased gradually to threshold then reduced again to a point where the patient is unable to feel paraesthesias regardless of the position
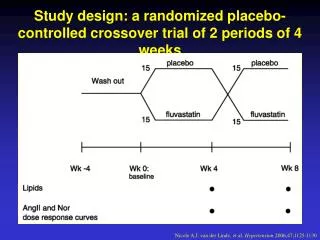
End of Study NS is restarted Randomisation Sequence 1 Patient Inclusion DATA 1 DATA 3 DATA 5 DATA 7 NS NS to HF HFtoNS NS toSham Sequence 2 DATA 2 DATA 4 DATA 6 DATA 8 NS NS toSham Shamto NS NS to HF Visit 1 Visit 2 Visit 3 Visit 4 Visit 5 Normal Stimulation 5 Day Data Collection DATA X HF Stimulation 5Khz Sham PGIC 2 week periods
Randomisation & Blinding • Randomisation • Subjects were randomised to receive sequence 1 or 2 using central randomisation service • Blinding Precautions • Research teams were split into 2 groups of blinded and unblinded personnel with no crossover in personnel • In patients with rechargeable devices we set an IPG current leakage in the sham period to similar level of the current usage during HFSCS • Patients were asked to guess the nature of the treatment they received to test the blinding strength at visits 3 and 5
Primary Outcome measure: PGIC • Patient Global Impression of Change (PGIC) • end of each 2-week period. "Since the last visit to the pain clinic my overall pain control is: • very much improved • much improved • minimally improved • no change • minimally worse • much worse • very much worse • A responder is defined as a subject reporting at least a “minimal improvement”, with the point of reference being the last visit under conventional stimulation
Study Flow 17 Completed Sequence 1 HF first 40 Patients Consented Patients Randomized 33 Patients Analysed Withdrawn 1 battery failure 1 lead fracture 2 withdrew consent 1 Battery flipping 16 Completed Sequence 2 Sham First 2 patient withdrew consent
Results: Sample Baseline Characteristics Data are mean (SD).
Results: Blinding • None of the subjects reported a sensation of paraesthesias in either group • At visit 3, the proportion of patients guessing their therapy group correctly was 15/33 = 45% • At visit 5 the proportion guessed correctly was 18/33 = 55%. • Neither is significantly different from chance (50%)
Results: Patient Global Impression of Change (PGIC) • In sequence 1 (HF first) 9/17 (52.9%) responded to HF vs. 2/17 (11.7%) to sham; a difference of (41.2%) • In sequence 2 (sham first) 5/16 (31.2%) responded to HF vs. 8/16 (50%) tosham; a difference of (18.8%, in favour of sham) • The overall treatment effect (benefit of HF vs. sham) is the average of these two proportions: (0.412 and -0.188) = 0.112 (11.2%)1. a responder is defined as a subject reporting at least a ‘minimal improvement’, with the point of reference being the last visit under conventional stimulation) 1. Schouten H, Kester A: A simple analysis of a simple crossover trial with a dichotomous outcome measure. Stat Med 2010; 29: 193-8.
The Period Effect • We observed a substantial period effect, irrespective of treatment received, with 17/33 (51.5%) patients benefiting at Visit 3 versus 7/33 (21.2%) at Visit 5; mean difference in proportions = 30%(P=0.006).
Conclusions I • This is the first double blinded RCT in spinal cord stimulation • We showed a minimal advantage of HF over sham as a proportion of 11.2% ( P=0.30). • We showed a substantial period effect with a greater proportion of responders at visit 3 versus visit 5 (difference = 30% P=0.006). • Both VAS & EQ-5D show the same consistent pattern of period effect (NS differences)
Conclusions II • At settings used, HF offers small advantage over sham. Only the order of the treatment in the sequence, dictates a significant effect • We believe this period effect to be related to patient expectation, or a “study” effect. • Study Limitation • These findings cannot be extrapolated to other stimulation frequencies/modes applied for a longer duration of time on stimulation naïve patients • We applied sub-threshold amplitudes; stimulation above sensory threshold may have been unpleasant and resulted in ublinding • The short duration of HFSCS and sham may have allowed a carry over effect of conventional SCS to play a significant role • Cathode position
Thankyou • Middlesbrough Team • A Gulve • G. Madzinga • F. Garner • S. West • M. Brookes • S. Eldabe • Morges Team • C. Perruchoud • A Durrer, • B. Rutschmann, • M. Rosato • N. Bovet • E. Buchser Prof. A. Batterham Teesside University
Thank You • Morges Team • C. Perruchoud • A Durrer, • B. Rutschmann, • M. Rosato • E. Buchser • Middlesbrough Team • A Gulve • G. Madzinga • F Garner • S. West • M. Brookes • S. Eldabe • Prof. A. Batterham Teesside University
Sample Size and statistical methods • Sample size • Using methods proposed by Schouten and Kester1, we estimated that a sample of 38 patients was required to have 90% power (2P=0.05) detect a difference in the proportion of patients responding to treatment in HF vs. sham of 25% • Statistical analysis • PGIC :methods of Schouten and Kester, in which the treatment difference (HFSCS-sham) for each of the two treatment sequences is computed and then averaged. • Pain VAS and EQ5-D index analysed using a conventional within-subjects model accounting for the period effect and utilizing the baseline scores before each treatment (visits 2 and 4) in an ANCOVA model 1. Schouten H, Kester A: A simple analysis of a simple crossover trial with a dichotomous outcome measure. Stat Med 2010; 29: 193-8.
Secondary Outcome measures • Pain VAS • mean pain VAS on the HF treatment was 4.35 cm vs. 4.26 cm on the sham (P=0.82). • Irrespective of treatment received, the mean VAS in the first treatment period (visit 3) was 3.99 cm vs. 4.63 cm in the second period (Visit 5) ; difference (visit 3 minus visit 5) = -0.64 cm (95% CI, -1.41 to 0.14 cm; P=0.11). Visit 3 VAS 3.99 Visit 5 VAS 4.63
Secondary Outcome Measures • MeanEQ5D-index on the HF treatmentwas 0.480 vs. 0.463on the sham; difference (HF minus sham) = 0.017 (95% CI, -0.101 to 0.135; P=0.78). • MeanEQ5-Dindex was 0.510 atvisit 3 vs. 0.432 atVisit 5; difference (visit 3 minus visit 5) = 0.078 (95% CI, -0.041 to 0.196 ; P=0.19). Visit 3 EQ5D 0.51 Visit 5 EQ5D 0.432