Download
1 / 14
140 likes | 193 Views
This guide covers the definition and etiology of FUO, including common causes such as infections, systemic inflammatory conditions, malignancies, and miscellaneous factors. It also delves into the diagnostic approach, investigation steps, and management of FUO cases. Additionally, it provides a detailed overview of HLH, including its pathophysiology, causes, suspicion, diagnosis criteria, and treatment options.

E N D
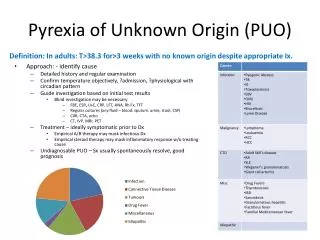
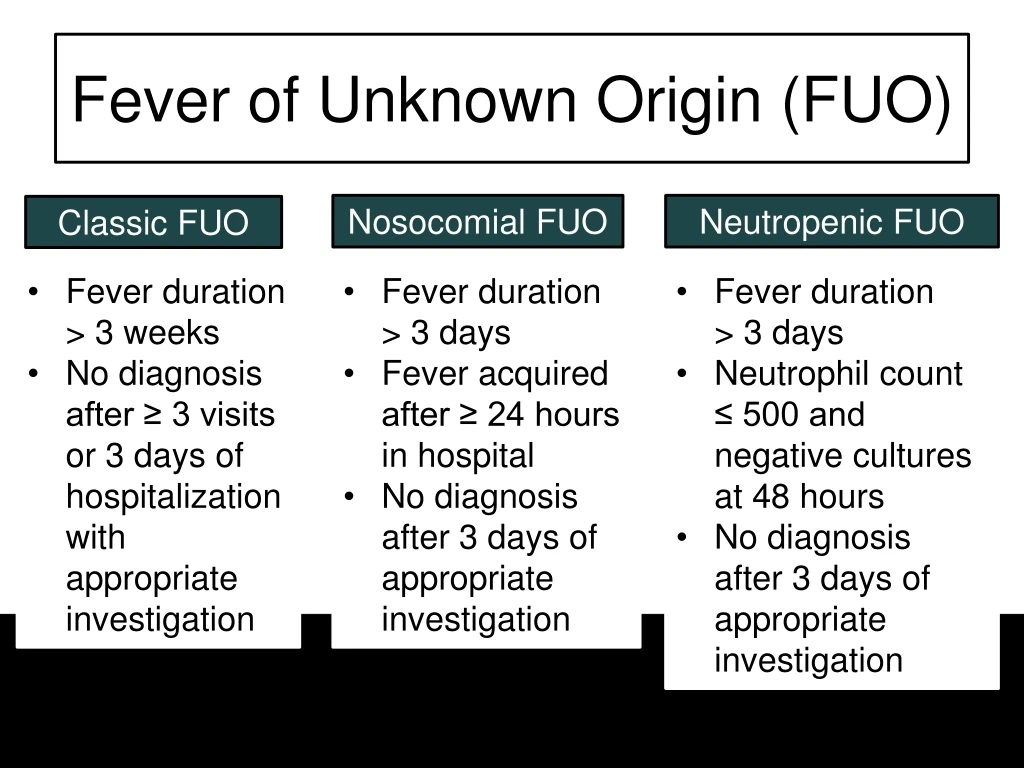
Fever of Unknown Origin (FUO) Nosocomial FUO Neutropenic FUO Classic FUO • Fever duration > 3 weeks • No diagnosis after ≥ 3 visits or 3 days of hospitalization with appropriate investigation • Fever duration > 3 days • Fever acquired after ≥ 24 hours in hospital • No diagnosis after 3 days of appropriate investigation • Fever duration > 3 days • Neutrophil count ≤ 500 and negative cultures at 48 hours • No diagnosis after 3 days of appropriate investigation
“Appropriate Investigation” Thorough history and physical exam Diagnostic testing Imaging Labs CXR • CBC with differential • Basic metabolic panel • Liver panel • Urinalysis, including microscopy and culture • Blood cultures
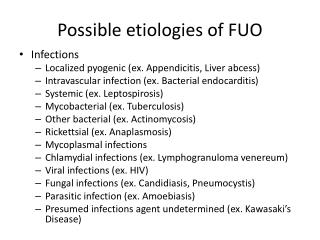
FUO: Etiology Infection Systemic Inflammatory Disease Malignancy Miscellaneous Causes
FUO: Infections Common Causes Account for about 20-40% of cases Abscess Endocarditis Tick-borne disease Tuberculosis Sinusitis Osteomyelitis CMV, EBV Complicated UTI
FUO: Systemic Inflammatory Young Adults Older Adults • Account for about 10-30% of cases • Common causes vary by age Still’s disease Temporal arteritis Rheumatoid arthritis variants Polymyalgia rheumatica SLE Others: polyarteritis nodosa, granulomatous diseases
FUO: Malignancies Common Causes • Account for 20-30% of cases • Fevers may persist for months or years Leukemia Lymphoma Renal cell carcinoma GI malignancies CNS malignancies Hepatocellular carcinoma
FUO: Miscellaneous Causes Reported Causes Account for 10-20% of cases Subacute thyroiditis Drug fever Pheochromocytoma Antimicrobials HLH Anticonvulsants Familial fevers NSAIDs NMS Cardiac meds
Next steps… Labs All patients: LDH, ESR, CRP, HIV, rheumatoid factor, ANA Risk factor specific: TB skin test or IGRA, SPEP/UPEP, blood smear, CMV serology, EBV serology, lumbar puncture, fungal culture, Q fever testing, Bartonella serology, Brucella serology, etc. Imaging All patients: CT chest and abdomen, echocardiogram Risk factor specific: head/spine imaging, venous duplex Biopsy? Therapeutic trials?
Hemophagocytic Lymphohistiocytosis Hemophagocytic = phagocytosis of blood cells and their precursors Histiocytoses = disorders in which accumulation of macrophages occurs Primary HLH Secondary HLH Children, often before 1 year of life. Genetic causes. Children and adults, many triggers. Some genetic predisposition (up to 14% adults with mutations). 50-75% mortality without prompt treatment. Even with treatment high mortality.
HLH Causes Up to 25% idiopathic. In adults, up to 50% due to malignancy. Autoimmune diseases Infections Viral: EBV, CMV, HIV, VZV, Influenza, Parvovirus, Hepatitis SLE, vasculitis, adult onset Still’s Malignancy Bacterial: Mycobacterium, Rickettsia, Babesia Prolonged stimulation of immune system prior, toll receptors involved? Lymphoma’s and leukemia’s, solid tumors Fungal: Histoplasmosis Malignant cell activation of proinflammatory cytokines, dysregulation of bone marrow, chemo affects *Macrophage-activating syndrome Parasitic: Leishmania, Plasmodium
HLH Suspicion and Diagnosis Potential lab findings: cytopenias, low fibrinogen, high ferritin, LP with elevated protein and lymphocytic pleocytosis 2004 Criteria: 5/8 required New (2005) Criteria for MAS: • Fever >38.5 • Splenomegaly • At least 2 cytopenias (hgb <9, platelets <100,000, neutrophils <1000) • Fasting TG’s >265 mg/dL • Fibrinogen <150 mg/dL • Elevated IL-2 CD25 2SD above ULN • Low or absent NK cell cytotoxic activity • Ferritin >500 • Hemophagocytosis in bone marrow, spleen, lymph node or liver • Platelet count <262 • AST >59 • WBC <4.0 • Fibrinogen <2.5 g/L • CNS dysfunction • Hemorrhages • Hepatomegaly
HLH Treatment Extensive search for underlying cause Corticosteroids +/- IVIG, *immunosuppressives Treat underlying cause *etoposide, intrathecal methotrexate for CNS, cyclophosphamide; rituximab in EBV, alemtuzumab (antibody against CD25), plasma exchange last line