Download
1 / 27
290 likes | 744 Views
Pathophysiology of Atherosclerosis. Dr Geer Mohammad Ishaq Senior Assistant Professor Department of Pharmaceutical Sciences University of Kashmir. Atherosclerosis.

E N D
Pathophysiology of Atherosclerosis Dr Geer Mohammad Ishaq Senior Assistant Professor Department of Pharmaceutical Sciences University of Kashmir For the exclusive use of Kashvarsity e-group members
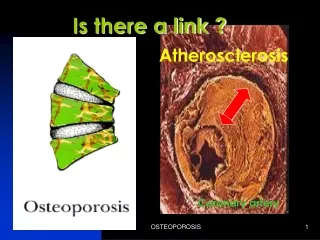
Atherosclerosis • Atherosclerosis is a specific form of arteriosclerosis (thickening & hardening of arterial walls) affecting primarily the intima of large and medium-sized muscular arteries and is characterized by the presence of fibrofatty plaques or atheromas. • The term atherosclerosis is derived from athero (meaning porridge) referring to the soft lipid-rich material in the centre of atheroma, and sclerosis (scarring) referring to connective tissue in the plaques.
Atherosclerosis • Most commonly affected arteries by atherosclerosis include large and medium sized arteries like aorta, coronary, popliteal and cerebral arteries. • Major complications resulting from ischemia due to atherosclerosis include myocardial infarction leading to heart attacks and cerebral infarction leading to strokes. • Less common complications include peripheral vascular disease, aneurysmal dilatation due to weakened arterial wall, chronic ischemic heart disease, ischaemic encephalopathy and mesenteric occlusion.
Etiology • Atherosclerosis is the cause of more than half of all deaths in the western industrialized nations. • Incidence progressively increasing in developing nations too in an epidemic proportion over the last few decades due to fast changing lifestyles. • Deaths from myocardial infarction (20-25 % of all deaths) are mostly related to underlying atherosclerosis. • Cardiovascular disease related to atherosclerotic coronary heart disease (CHD) or ischaemic heart disease (IHD) is the most common cause of death in the developed countries of the world.
Risk Factors in Atherosclerosis Major risk factors 1) Major Constitutional risk factors: i. Age ii. Sex iii. Genetic factors iv. Familial and racial factors 2) Major Acquired risk factors: i. Hyperlipidaemia ii. Hypertension iii. Diabetes mellitus iv. Smoking v. Hyperhomocysteinemia
Risk Factors in Atherosclerosis Minor Risk Factors: 1. Environmental influences 2. Obesity 3. Hormones: Oestrogen deficiency, oral contracep. 4. Physical inactivity 5. Stressful life 6. Infections (C. pneumoniae, Herpes virus, CMV) 7. Homocystinuria 8. Role of Alcohol
Major Constitutional Risk Factors AGE • Atherosclerosis is an age-related disease. • Clinically significant lesions are found with increasing age. • Fully-developed atheromatous plaques usually appear in 40s and beyond. • Evidence in support comes from the high death rate from IHD in this age group.
Major Constitutional Risk Factors SEX • Incidence and severity of atherosclerosis is more in men than in women. • Prevalence of atherosclerotic IHD is about three times higher in men in 4th decade than in women. • Lower incidence of IHD in women, especially in premenopausal age is probably due to high levels of oestrogens and high-density lipo- proteins, both of which have anti-atherogenic influence.
Major Constitutional Risk Factors GENETIC FACTORS • Hereditary genetic derangements of lipoprotein metabolism predispose the individuals to high blood lipid level and familial hypercholesterolaemia. FAMILIAL AND RACIAL FACTORS • Familial predisposition to atherosclerosis may be related to other risk factors like diabetes, hypertension and hyperlipoproteinaemia. • Racial differences too exist. Blacks have less severe atherosclerosis than Whites.
Major Acquired Risk Factors HYPERLIPIDAEMIA Hypercholesterolaemia has directly proportionate relationship with atherosclerosis and IHD because: • The atherosclerotic plaques contain cholesterol and cholesterol esters largely derived from the lipoproteins in the blood. • The lesions of atherosclerosis can be induced in experimental animals by feeding them cholesterol-rich diet. • Individuals with hypercholesterolaemia due to various causes such as diabetes mellitus, myxoedema, nephrotic syndrome and familial hypercholesterolaemia have increased risk of developing atherosclerosis and IHD. • Populations having hypercholesterolaemia have higher mortality from IHD. Dietary regulation and administration of cholesterol-lowering drugs have beneficial effect on reducing the risk of IHD
Major Acquired Risk Factors HYPERLIPIDAEMIA • Virchow in 19th century first identified cholesterol crystals in the atherosclerotic lesions. • An elevation of serum cholesterol levels above 260mg/dl in men and women between 30 and 50 years of age has three times higher risk of developing IHD as compared with people with normal serum cholesterol levels (140-200 mg/dl). • Low-density lipoproteins (LDL) is richest in cholesterol and has maximum association with athersc • VLDL carries much of triglycerides & has less marked effect than LDL. • HDL is protective good cholesterol against atherosclerosis. • Diet rich in saturated fats e.g., eggs, meat, milk, butter etc raises the plasma cholesterol level while the diet rich in poly-unsaturated fats and omega-3 fatty acids e.g., fish, fish oils etc lowers its level.
Major Acquired Risk Factors HYPERTENSION • Hypertension causes mechanical injury to the arterial wall due to increased blood pressure leading to athero-sclerotic IHD and cerebrovascular disease. • Endothelial injury due to persistent high B.P leads to plaque formation as per response to injury hypothesis. • A systolic pressure of over 160 mmHg or a diastolic pressure of over 95 mmHg leads to 5 times higher risk of developing IHD than in people with normal B.P. (140/90 mmHg or less).
Major Acquired Risk Factors SMOKING • The extent and severity of atherosclerosis are much greater in smokers than in non-smokers. • Cigarette smoking is associated with higher risk of atherosclerosis, IHD and sudden cardiac death. • Increased risk is due to reduced level of HDL and accumulation of carbon monoxide in the blood that produces carboxy-haemoglobin and eventually hypoxia in the arterial wall favouring atherosclerosis. • Smoking also promotes Athr. by increased platelet adhesiveness, raised endothelial permeability, symapathetic nervous system stimulation by nicotene.
Major Acquired Risk Factors DIABETES MELLITUS • Atherosclerosis develops at an early age in people with both insulin-dependent and non-insulin dependent diabetes mellitus. • The risk of cerebrovascular disease is high and frequency to develop gangrene of foot is about 100 times increased. • Causes of increased severity of Ath. are complex and include increased aggregation of platelets, increased LDL and decreased HDL.
Minor Risk Factors • Higher incidence of Athr. in developed countries is primarily because of environmental influences. • Obesity: Risk is increased if a person is overweight by 20% or more. • Use of exogenous hormones like oral contraceptives by women or endogenous oestrogen deficiency e.g., in post-menopausal women leads to increased risk. • Physical inactivity and lack of exercise increases risk • Stressful life style led by aggressiveness, competitive drive, over-ambitiousness and a sense of urgency is associated with enhanced risk of IHD.
Minor Risk Factors 6. Infections particularly Clamydia pneumoniae and viruses such as herpesvirus and cytomegalovirus increases coronary atherosclerotic lesions. 7. Patients with homocystinuria, an inborn error of metabolism have early athr and CAD. 8. Moderate consumption of alcohol has slightly beneficial effect by raising the level of HDL cholesterol and by causing vasodilation. 9.However persistent consumption of alcohol in large quantities causes more damage.
Pathogenesis of Atherosclerosis INSUDATION HYPOTHESIS Put forth by Virchow in 1852 stating that Ath is a form of cellular proliferation of the intimal cells resulting from increased imbibing of lipids from the blood. Earlier known as “lipid theory” is now called “response to injury hypothesis” and is the most widely accepted theory. ENCRUSTATION HYPOTHESIS Put forth by Rokitansky in 1852 stating that atheroma represented a form of encrustation on the arterial wall from the components in the blood forming thrombi composed of platelets, fibrin and leucocytes, and was earlier named as “thrombogenic theory”.
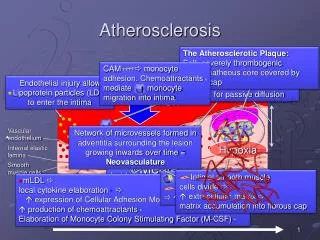
Response to Injury Theory • Original theory put forth in 1973 modified in 1993. • Original Theory: Initial event in atherogenesis is endothelial injury followed by smooth muscle cell proliferation. As per this theory early lesions mainly consist of smooth cells. • Modified theory describes lipoprotein entry into the intima as the initial event followed by lipid accumulation in the macrophages (now foam cells) which according to modified theory are the dominant cells in early lesions.
Monoclonal Hypothesis • Based on the postulate that proliferation of smooth muscle cells is the primary event and that this proliferation is monoclonal in origin similar to cellular proliferation in neoplasms. • Evidence in support of this hypothesis is the presence of proliferated smooth muscle cells in atheromatous plaques which have only one of the two forms of G6PD isoenzymes, suggesting monoclonality in origin. • Monoclonal proliferation of smooth muscle cells in Ath. may be initiated by mutations caused by exogenous chemicals like cigarette smoke or endogenous metabolites like lipoprotiens or some viruses like herpesvirus.
Progression of Atherosclerosis • Endothelial Injury: • Initial triggering event in the development of Atherosclerotic lesions • Causes ascribed to endothelial injury in experimental animals include mechanical trauma, haemodynamic forces, immunological and chemical mechanisms, metabolic agents like chronic hyperlipidaemia, homocystine, circulating toxins from systemic infections, viruses, hypoxia, radiation, carbon monoxide and tobacco products. • In man, two major risk factors are haemodynamic stress from hypertension and chronic hyperlipidaemia.
Progression of Atherosclerosis • Intimal Smooth Muscle Cell Proliferation • Endothelial injury causes adherence aggregation and platelet release reaction at the site of exposed subendothelial connective tissue. • Proliferation of intimal smooth muscle cells is stimulated by various mitogens released from platelets adherent at the site of endothelial injury. • These mitogens include PDGF, fibroblast growth factor, TGF-ά. • Proliferation is also facilitated by nitric oxide and endothelin released from endothelial cells.
Progression of Atherosclerosis 3. Role of Blood Monocytes • Though blood monocytes do not possess receptors for normal LDL, LDL does appear in the monocyte cytoplasm to form foam cell. • Plasma LDL on entry into the intima undergoes oxidation. Oxidised LDL formed in the intima performs following two important functions : • For monocytes, oxidized LDL acts to attract, proliferate, immobilise and activate them and is readily taken up by scavenger receptor on the monocyte to transform it to a lipid laden foam cell. • For endothelin, oxidized LDL is cytotoxic.
Progression of Atherosclerosis 4. Role of Hyperlipidaemia • Chronic hyperlipdaemia in itself may initiate endothelial injury and dysfunction by casing increased permeability. • Increased serum concentration of LDL and VLDL promotes formation of foam cells, while high serum concentration of HDL has anti-atherogenic effect.
Progression of Atherosclerosis 5. Thrombosis • Endothelial injury exposes sub-endothelial connective tissue resulting in platelet aggregation at the site besides proliferation of smooth muscle cells. • This causes mild inflammatory reaction which together with foam cells is incorporated into atheromatous plaque. • Lesions enlarge by attaching fibrin and blood cells causing thrombus formation which becomes a part of atheromatous plaque.