Download
1 / 41
430 likes | 683 Views
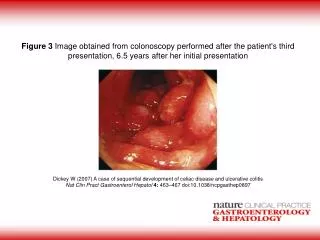
Acute Pediatric Ulcerative Colitis: Lessons from the OSCI Trial. James Markowitz, MD Professor of Pediatrics Hofstra – North Shore LIJ School of Medicine Department of Pediatrics Cohen Children’s Medical Center of NY New Hyde Park, NY. Disclosures.

E N D
Acute Pediatric Ulcerative Colitis: Lessons from the OSCI Trial James Markowitz, MD Professor of Pediatrics Hofstra – North Shore LIJ School of Medicine Department of Pediatrics Cohen Children’s Medical Center of NY New Hyde Park, NY
Disclosures I have the following financial relationships : Janssen Biotech: research support, consultant UCB: consultant Abbvie: consultant
Acute Severe Colitis in Adults(European Crohn’s and Colitis Organization, 2008) At least six bloody stools per day and at least one of the following: Tachycardia ( > 90 b.p.m.) Temperature > 37.8 ° C Anemia (hemoglobin < 10.5 g/ dl) Elevated ESR ( > 30 mm/ h) Travis SPL, et al. J Crohn Colitis 2008;2 :24-62
Pediatric UC Activity Index (PUCAI) Turner D, et al. Gastroenterology 2007;133:423-32.
PUCAI cutoffs (n=205) r=0.91 P<0.001 Definition AUC of ROC Sens/Spec 0.97 (0.95-0.99) 96%/ 91% Severe: >65 n=25 96%/ 91% 0.97 (0.95-0.99) Mod: 35-60 PUCAI score n=57 n=42 0.98 (0.97-0.99) 89%/ 94% Mild: 10-30 0.99 (0.99-1) 95%/ 99% None: <10 n=81 None Moderate Severe Mild Turner D et al; Gastroenterology 2007;133:423-432
Acute Severe Colitis: Frequency • Adults: 18-25% of patients over 10 years Edwards FC, Truelove SC. Gut. 1963 Dec;4:299-315. Dinesen LC, et al. J Crohn Colitis. 2010 Oct;4(4):431-7. Epub 2010 Feb 19. • Children: • Retrospective review of admissions to Hospital for Sick Children in Toronto (1991-1996) • “Population based” sample estimate (only children with addresses from the Greater Toronto area) • 55/196 (28%) of children with UC <15 yrs of age admitted for IV corticosteroids Turner D, et al. Gut. 2008 Mar;57(3):331-8.
Natural History of UC:Looking back the picture was not pretty 1BMJ 1933;2:812; 2BMJ 1955;4947:1041; 3Arch Dis Child 1973;48:337; 4J Clin Gastroenterol 1979;1:301; 5Gastroenterology 1994;107:3
Cumulative Probability of Colectomy In Children with UC (1975-1995) Hyams JS et al. J Pediatr. 1996;129:81. Mild vs moderate/severe, P<0.03
Cumulative Probability of Colectomy in Children with UC (1975-1995) 0.4 0.3 0.2 0.1 0.0 Moderate/Severe (n=98) Mild (n=73) 26% Cumulative Probability 9% • 0 1 2 3 4 5 6 7 Years From Diagnosis Hyams JS et al. J Pediatr. 1996;129:81. Mild vs moderate/severe, P<0.03
How might we change the outcome of children with acute severe colitis?
Severe/Fulminant Ulcerative Colitis 16 year old presents with 10 bloody stools per day, Hb 9, unresponsive to oral corticosteroids
What is the OSCI Trial? OSCI = Outcome of Steroid therapy in Colitis Individuals
How effective are intravenous corticosteroids for acute severe UC?
IV Corticosteroids for Acute Severe UC OSCI 2008-2009 (prospective) Study population N=128 IV Steroid Failure N=37 (29%) IV Steroid Success N=91 (71%) Turner D et al Gastro 2010;138(7):2282-91 Toronto 1991-2000 (retrospective) Study population N=99 IV Steroid Failure N=46 (46%) IV Steroid Success N=53 (53%) Short term: 53% avoid colectomy &/or rescue therapy 1 Year: 18% steroid free without colectomy &/or rescue therapy Short term: 71% avoid colectomy &/or rescue therapy 1 Year: 59% steroid free without colectomy &/or rescue therapy Turner D et al. Gut 2008; 57:331-338
What factors predict likely response to intravenous corticosteroids (IVCS)?
Predictors of IV Corticosteroid Response on Day 0: OSCI Trial Turner D et al Gastro 2010;138(7):2282-91
How long should we wait for intravenous corticosteroids to be effective?
Duration of Initial Therapy • Recommendations vary, depends upon absence of absolute indications for surgery • If you wait too long complications will occur • 7 days1,2 • 10 to 14 days3,4 • >14 days is acceptable5 • Treatment for 15 to 36 days • 1 patient to surgery, perforation, 11 units packed RBC 4Meyers S. J Clin Gastroenterol. 1990 Aug;12(4):479-80 5Gold et al. Am J Gastroenterol. 1995 May;90(5):732-5. 1Truelove SC et al. Lancet. 1974;1:1067. 2Goligher JC et al. Br Med J. 1970 Dec 19;4(737):703-6. 3Werlin SL et al. Gastroenterology. 1977;73:828.
Predicting IV Corticosteroid Failure and Need for Rescue Therapy Day 3: PUCAI >45 (moderate) – start planning Day 5: PUCAI >70 (severe) – time for 2nd line Rx Turner D et al Gastro 2010;138(7):2282-91
Time to 2nd Line Therapy Stratified by PUCAI on Day 3 and Day 5 Turner D et al Gastro 2010;138(7):2282-91
What therapy is best when iv corticosteroids fail? Calcineurin inhibitors (cyclosporine, tacrolimus) vs Anti-TNF (infliximab)
Multicenter 14 patients Prospective, open-label 10 UC, 2 CD, 2 IC Minimum 7 days of severe colitis despite CS Acute response: 13/14 (93%) Colectomy by 1 yr: 8/13 (62%) Tacrolimus in Peds UC UCLA • 18 patients • Retrospective, open-label • 9 steroid resistant UC • Acute response: 8/9 (89%) • Colectomy by 1 yr: 6/9 (67%) Ziring at al. JPGN 2007;45(3):306-311. Bousvaros A et al. J Pediatr. 2000;137:794
Tacrolimus Pediatric Experience (Boston Children’s) • 46 children, retrospective, open-label • All steroid refractory UC • 43/46 (93%) acute response • 60% colectomy at 26 months Watson S et al. Inflamm Bowel Dis. 2011 Jan;17(1):22-9. Epub 2010 Aug 18
Infliximab Induction in Chronic Active UC Pediatric trial Adult trials Open label induction with 5 mg/kg infliximab at 0, 2, 6 weeks Treatment outcome assessed at 8 weeks Hyams J et al. Clin Gastroenterol Hepatol 2012;10(4):391-9 Rutgeerts P, at al. N Engl J Med 2005;353:2462-76
Infliximab in Acute Severe Colitis • Swedish double-blind placebo controlled adult UC trial • 24 infliximab, 21 placebo • 3 month colectomy rates • Infliximab: 7/24 (29%) • Placebo: 14/21 (67%) (P = .017; odds ratio, 4.9; 95% confidence interval, 1.4-17) Jarnerot G, et al. Gastroenterol. 2005 Jun;128(7):1805-11
2nd Line Rx for Acute Severe UC:Infliximab OSCI 2008-2009 (prospective) Short Term Response to Infliximab: 25/33 + 5/7 = 30/40 (75%) avoid imminent colectomy Response at 1 Year 18/33 + 5/7 = 23/40 (58%) avoid colectomy Study population N=128 IV Steroid Failure N=37 (29%) IV Steroid Success N=91 (71%) Infliximab N=33 Infliximab N=7 Colectomy N=3 Acute Outcome Response N = 25 Colectomy N = 8 Cyclosporine N=1 Colectomy N=3 Outcome at 1 Year Response N = 5 Colectomy N = 2 Outcome at 1 Year Colectomy N = 7 Turner D et al Gastro 2010;138(7):2282-91
Colectomy Following Rescue Therapy for IVCS Resistant Acute Severe Colitis Turner D et al Gastro 2010;138(7):2282-91 Turner D et al. Gut 2008; 57:331-338 Ziring at al. JPGN 2007;45(3):306-311 Bousvaros A et al. J Pediatr. 2000;137:794 Watson S et al. IBD 2011;17(1):22-9
Colectomy Following Rescue Therapy for IVCS Resistant Acute Severe Colitis Turner D et al Gastro 2010;138(7):2282-91 Turner D et al. Gut 2008; 57:331-338 Ziring at al. JPGN 2007;45(3):306-311 Bousvaros A et al. J Pediatr. 2000;137:794 Watson S et al. IBD 2011;17(1):22-9
Cyclosporine vs Infliximab in Acute Severe UC: A parallel, open-labelrandomised controlled adult trial Patients (N=115) Severe, acute UC IV steroid resistant Treatments IV CsA (2 mg/kg/d x 1 week, then po x 98 days) IFX (5mg/kg at 0-2-6 wks) In patients with a clinical response at week 7, azathioprine initiated and steroids decreased Laharie D et al. Lancet 2012; 380: 1909–15
What else can we do to decrease colectomy rates further? Remember to look for: C. Difficile CMV Why are today’s outcomes following iv steroids better than in the past?
C difficile Complicating IBD • C diff prevalence in hospitalized children • IBD (24.7%) vs non-IBD controls (8.9%) OR 3.3 (95%CI 1.5 to 7.6) Pascarella F, et al. J Pediatr. 2009 Jun;154(6):854-8 • Compared to adults with either condition alone, those with both C diff and IBD have • lengthier hospitalizations • fourfold increased mortality Ananthakrishnan AN, McGinley EL, Binion DG. Gut. 2008 Feb;57(2):205-10
C difficile and IBD • Diagnosis • Immunoassays or ELISAs for toxin A and toxin B • Cytotoxicity assay • PCR • Diagnostic accuracy • One toxin assay fails to identify most infections • Toxin A assay missed 41.5% of infections • Toxin B assay missed 34.9% of infections Markowitz JE, et al. Am J Gastroenterol. 2001 Sep;96(9):2688-90
C difficile Can be Difficult to Diagnose in IBD Despite Assay for Both Toxin A and B Issa M, et al. Clin Gastroenterol Hepatol. 2007 Mar;5(3):345-51
CMV Complicating UC • CMV disease = CMV in tissue • Sigmoidoscopy and Bx • Immunohistochemistry better than light micro • Patient characteristics • Seropositive; Immunosuppressed • Effects: steroid resistance • 5-36% of CS resistant UC vs 0-10% with CS sensitive UC • Rx: Gangcyclovir, ?d/c immune suppression rihes.cmu.ac.th markwickmd.com Dommenech E, et al. Inflamm Bowel Dis 2008;14:1373–1379
Lessons of the OSCI Study Acute severe colitis continues to present significant clinical challenges Colectomy: 9% acutely, 19% at 1 year Use PUCAI to judge severity of disease and response to therapy PUCAI >45 on Day 3 → plan rescue Rx …(flex sig for CMV) PUCAI ≥70 on Day 5 → time for 2nd line treatment
Both infliximab and calcineurin inhibitors Can induce remission in ~75% of children with steroid resistant severe acute colitis Can avoid colectomy long term in 40-60%
Fulminant UC is still a very difficult group to treat Surgery will never be an attractive alternative for most patients, but for some there is no choice We need more data on how to treat our patients