Download
1 / 31
320 likes | 1.24k Views
AHLTA. Data Quality Management Course September 15-17, 2009. DHIMS Sustainment . How Provider Workload is Measured. Provider productivity is measured by RVU’s. These are determined primarily by 2 components: The E&M (Evaluation and Management) Code And Procedures (CPT and HCPCS codes).

E N D
AHLTA Data Quality Management Course September 15-17, 2009 DHIMS Sustainment
How Provider Workload is Measured • Provider productivity is measured by RVU’s. These are determined primarily by 2 components: • The E&M (Evaluation and Management) Code • And Procedures (CPT and HCPCS codes)
E&M/RVU Considerations Not all clinics are created equal • Primary Care and Family Practice are DIFFERENT clinics New patients earn more RVU’s than established ones • Some sample E&M/RVU pairs: • E&M code (explanation) New pt Est pt: • 99212 (Problem Focused) 0.45 0.45 RVU • 99213 (Expanded Problem Focused) 0.88 0.67 RVU • 99214 (Moderate Complexity) 1.34 1.10 RVU • 99215 (High Complexity) 2.67 1.77 RVU • 99381/91 (Preventive Medicine 0-1 y. o.) 1.19 1.02 RVU • 99382/92 (Preventive Medicine 1-11 y. o.) 1.36 1.19 RVU • 99385/95 (Preventive Medicine 18-39 y. o.) 1.53 1.36 RVU • 99386/96 (Preventive Medicine 40-64 y. o.) 1.88 1.53 RVU
What About Procedures? Correct documentation of procedures is ESSENTIAL! Procedure RVU’s are added to the RVU’s generated by the E&M code • Ex: Visit for impaired hearing • (E&M 99213 RVU = 0.67) + ear wax removal (RVU = 0.61). TOTAL = 1.28 RVU • IMPORTANT: Providers can receive credit for procedures done by ancillary staff Place commonly done procedures in your order set for easy finding Make pre-coded “pre-text” forms to ensure complete and uniform documentation (and correct E&M coding!)
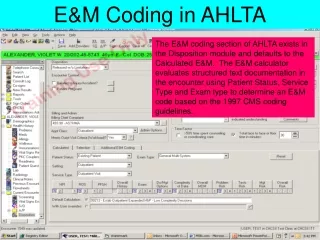
Provider Documentation Considerations • 838 doesn’t count anything outside of the S/O and AP modules in its automatic E&M calculations • Therefore, for example, vital signs entered by a technician in the VS module aren’t counted even though CMS rules allow this • This led to chronic under-coding • 3.3 counts all CMS-allowed items, leading to more accurate automatic coding
How an E&M Code is Determined • The visit is made up of 3 components: • Patient History (“S” = Subjective) • History of Present Illness (HPI) • Past Medical History (PMH) • Includes Family and Social History • Review of Systems (ROS) • Physical Examination (“O” = Objective) • Medical Decision Making (“A/P”, Assessment and Plan • Diagnosis/management risk • Complexity of data • Problem risk • Test risk • Management risk
How an E&M Code is Determined Component: Established Patient New Patient E&M 99213 99214 99202 99203 RVU 0.67 1.10 0.88 1.34 # Terms in HPI: 1-3 4 4 4 PMH: 0 1 1 3 ROS: 1 2 2 10 Note that if all the symptoms are clustered in the same module, the application will assign a lower E&M code, even though CMS doesn’t care where terms are placed
How an E&M Code is Determined • For Physical Examination • Problem Focused: • 1-5 “bullets’ (terms) from 1 or more body areas • Expanded Problem Focused: • 6 bullets from 1 or more body areas • Detailed: • 2 bullets from 6 or more body areas • Comprehensive: • 2 bullets from 9 body areas • Confusing? Yep… • “It’s not what I went to med school for”
Using a Utility AIM Form to Obtain Optimal (Correct) E&M Codes • More terms (e.g. symptoms, exam findings) is not always better • It’s where you place the terms that counts. Therefore, • Make the Electronic Record do the placing of terms for you • Allow the provider to shape the note to allow easier reading of the patient’s condition, not to “maximize” the code
Free-text Entry of HPI • For maximum coding credit (“Extended”, or 2 points), the HPI needs at least 4 of 8 items; location (of injury), quality (of symptoms), severity, duration, timing, context,modifying factors and associated signs or symptoms • The technician has already logged the severity of any pain in the VS module, and the injury location in the Screening module
Free-text Entry of HPI • It doesn’t take much to get 4 items • “Tripped over cat (context) 1 hour ago (timing), twisted ankle…” [the technician had already noted 4/10 pain (severity) in left ankle (location)] • “Began runny nose (location) and cough 2 days ago (duration), no fever (assoc. symptom), some response to GGDM syrup (modifying factor) • Most providers will document much more than that normally • In case of an intentionally brief, focused HPI, click the “X” to reduce the point number to one.
One-Click Entry of PMH Items • Medications and Problem list can be viewed instantly by clicking on the Health History tab, lower left • Verify the medications with the patient (reconciliation), then (usually the nurse) can click the “Medication list reviewed…” box • Other boxes can be checked/filled in as appropriate for medical documentation, but no further E&M credit is gained.
Example of Health History Summary PanelHover mouse pointer over the Health History tab at lower left
Documenting ROS by Exception • Most ROS items are negative anyway • Most patients aren’t being seen for infectious diseases • Infectious symptoms are separated out for one-click negation by themselves • It is fastest to click “All Normal”, then unclick those with abnormalities or those you didn’t ask about • Note how the form automatically assigns terms to the appropriate locations in the note for proper E&M coding
Rapid Entry of Normal PE FindingsUse for “Pertinent Negatives”
Rapid Entry of Normal PE Findings • Be sure to document only what you did look at or hear • You can hit “Normal” and then change the box in front of the one finding you did notice (e.g. heart sounds are all normal except for a murmur) • You can document details in free-text • Number in brackets indicates maximum number of terms that are creditable • Again, though, document what is needed for medical care!
More Detailed PE FindingsOften can enter findings by click faster than typing
Procedure-Specific Pre-Texted FormatsPre-coded fill-in-the-blank texts
Advantages of Utility Form • Often faster to enter data by click than by typing (though not necessarily than by dictation with Dragon) • Emitted note is segmented for easier reading • Terms are distributed for maximum (proper, non-padded) E&M code • Provider doesn’t need to know anything about E&M coding
Workflow Considerations • Documentation is a team effort • Technician should fill out Screening and VS modules • Nurse (or technician) should fill out HPI and ROS portions of form • When the provider enters, the note should be 2/3 done • Only have the provider do what only the provider can do
Issues raised at last DQ meeting • These were issues noted on the feedback forms turned in after the last meeting • Yes, we do read them
How to Fix ADM • ADM Errors are varied and have varied causes and solutions • ADM Error Codes and fixes are located on the Field Services website • https://fieldservices2.saic.com/Report.aspx?Id=941 • Tier 3 is working on an updated version • If desired, TIER 3 can requeue items that have not crossed. • 120 error codes can be ignored. The 120 designation indicates a fixed ADM writeback error.
Reports in AHLTA for DQ Analysis • The data quality reports and tools are available on the Field Services Website • https://fieldservices2.saic.com/Report.aspx?Id=941 • The reports available are: • AHLTA ADM Writeback Exception report • Appointments with No ADM Records by Clinic • ADM Patients with 3rd Party Insurance • ADM Compliance Report • ADM Records with Unresolved Coding Issues • Interface Transmission Status of ADM Record • Patient Encounter Records Report • ADM SADR/TPOCS Extract Status Display • ADM SADR Error Report • These should be run by the DQ Manager at Site. • If Site is having difficulty running the reports, please submit a Trouble Ticket for Tier 3.
Rules for Pseudo-SSN Use • Newborns • Require pseudo-SSNs until a SSN has been assigned. • John Does • EWSR Phase 1 release notes Section 5.3: The John Doe option allows you to register a patient whose identity is unknown. Once the patient's identity is determined, you can update the registration data using the Registration option. For this type of registration, the system automatically inserts DOE,JOHN(#) as the patient name, 99 (All others, not elsewhere classified) as the FMP, and a pseudo SSN (8xxx-xx-xxxx). The JOHN DOE COUNTER (#) is assigned by the system based on a John Doe Count function that increments by one for each new John Doe entered (i.e., DOE,JOHN17; DOE,JOHN18) and is stored in the ADT PARAMETERS file."