Download
1 / 1
10 likes | 158 Views
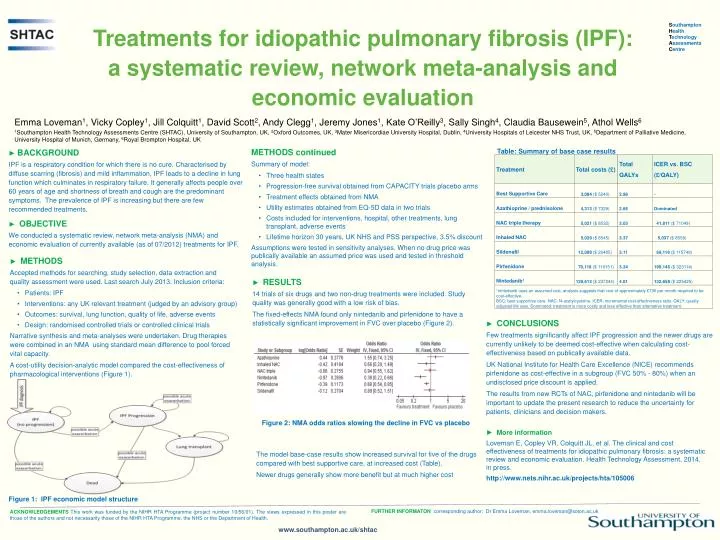
S outhampton H ealth T echnology A ssessments C entre. Treatments for idiopathic pulmonary fibrosis (IPF ): a systematic review, network meta-analysis and economic evaluation.

E N D
Southampton Health Technology Assessments Centre Treatments for idiopathic pulmonary fibrosis (IPF): a systematic review, network meta-analysis and economic evaluation Emma Loveman1,Vicky Copley1, Jill Colquitt1, David Scott2, Andy Clegg1, Jeremy Jones1, Kate O’Reilly3, Sally Singh4, Claudia Bausewein5, Athol Wells6 1Southampton Health Technology Assessments Centre (SHTAC), University of Southampton, UK, 2Oxford Outcomes, UK, 3Mater Misericordiae University Hospital, Dublin, 4University Hospitals of Leicester NHS Trust, UK, 5Department of Palliative Medicine, University Hospital of Munich, Germany, 6Royal Brompton Hospital, UK • METHODS continued • Summary of model: • Three health states • Progression-free survival obtained from CAPACITY trials placebo arms • Treatment effects obtained from NMA • Utility estimates obtained from EQ-5D data in two trials • Costs included for interventions, hospital, other treatments, lung transplant, adverse events • Lifetime horizon 30 years, UK NHS and PSS perspective, 3.5% discount • Assumptions were tested in sensitivity analyses. When no drug price was publically available an assumed price was used and tested in threshold analysis. Table: Summary of base case results ► BACKGROUND IPF is a respiratory condition for which there is no cure. Characterised by diffuse scarring (fibrosis) and mild inflammation, IPF leads to a decline in lung function which culminates in respiratory failure. It generally affects people over 60 years of age and shortness of breath and cough are the predominant symptoms. The prevalence of IPF is increasing but there are few recommended treatments. ► OBJECTIVE We conducted a systematic review, network meta-analysis (NMA) and economic evaluation of currently available (as of 07/2012) treatments for IPF. • ► METHODS • Accepted methods for searching, study selection, data extraction and quality assessment were used. Last search July 2013. Inclusion criteria: • Patients: IPF • Interventions: any UK relevant treatment (judged by an advisory group) • Outcomes: survival, lung function, quality of life, adverse events • Design: randomised controlled trials or controlled clinical trials • Narrative synthesis and meta-analyses were undertaken. Drug therapies were combined in an NMA using standard mean difference to pool forced vital capacity. • A cost-utility decision-analytic model compared the cost-effectiveness of pharmacological interventions (Figure 1). ► RESULTS 14 trials of six drugs and two non-drug treatments were included. Study quality was generally good with a low risk of bias. The fixed-effects NMA found only nintedanib and pirfenidone to have a statistically significant improvement in FVC over placebo (Figure 2). ► CONCLUSIONS Few treatments significantly affect IPF progression and the newer drugs are currently unlikely to be deemed cost-effective when calculating cost-effectiveness based on publically available data. UK National Institute for Health Care Excellence (NICE) recommends pirfenidoneas cost-effective in a subgroup (FVC 50% - 80%) when an undisclosed price discount is applied. The results from new RCTs of NAC, pirfenidone and nintedanib will be important to update the present research to reduce the uncertainty for patients, clinicians and decision makers. Figure 2: NMA odds ratios slowing the decline in FVC vs placebo ► More information Loveman E, Copley VR, Colquitt JL, et al. The clinical and cost effectiveness of treatments for idiopathic pulmonary fibrosis: a systematic review and economic evaluation. Health Technology Assessment, 2014, in press. http://www.nets.nihr.ac.uk/projects/hta/105006 The model base-case results show increased survival for five of the drugs compared with best supportive care, at increased cost (Table). Newer drugs generally show more benefit but at much higher cost Figure 1: IPF economic model structure FURTHER INFORMATON corresponding author: Dr Emma Loveman, emma.loveman@soton.ac.uk ACKNOWLEDGEMENTS This work was funded by the NIHR HTA Programme (project number 10/56/01). The views expressed in this poster are those of the authors and not necessarily those of the NIHR HTA Programme, the NHS or the Department of Health. www.southampton.ac.uk/shtac