Download
1 / 13
130 likes | 149 Views
Explore the characteristics, immune responses, and symptoms of hypersensitivities, including the four types and their effects. Learn about the factors affecting predisposition, treatments, and different types of hypersensitivity reactions. Discover the immune system involvement and effects on the body.

E N D
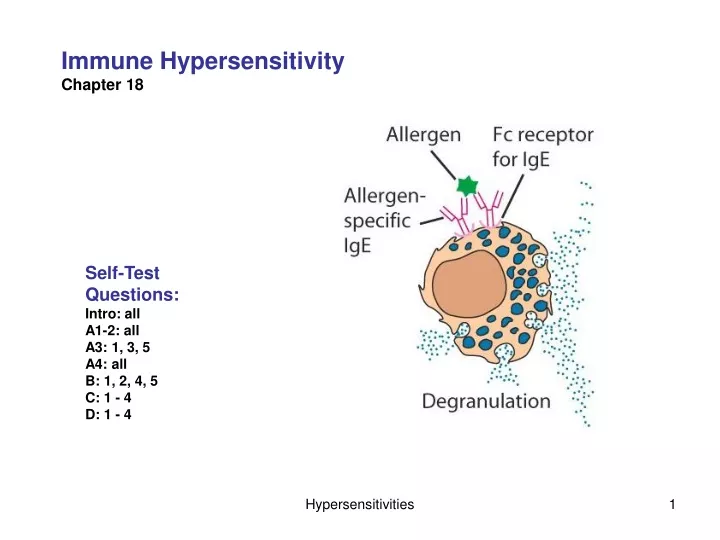
Immune Hypersensitivity Chapter 18 Self-Test Questions: Intro: all A1-2: all A3: 1, 3, 5 A4: all B: 1, 2, 4, 5 C: 1 - 4 D: 1 - 4 Hypersensitivities
What characteristics are shared by all hypersensitivies? Immune responses: Primary (sensitization) response Secondary (activation) response Abnormal (hyper-) response to antigens (allergens) Symptoms: localized or systemic Onset can be: Early, Late or Chronic Hypersensitivities
What are hypersensitivities? 4 types of hypersensitivities (Gel and Combs classification) Immune Namesystem involvedEffectorsEffectsOnset Type 1 “Atopic” Humoral (IgE) mast cells inflammation seconds eosinophils (anaphylaxsis) Type II “Cytotoxic” Humoral/ macrophages cell destruction hours Complement complement (hemolysis) Type III “Im. Complex” Humoral/ granulocytes inflammation hours Complement Type IV “Delayed type” Cell-mediated macrophages inflammation days -- TH1 Hypersensitivities
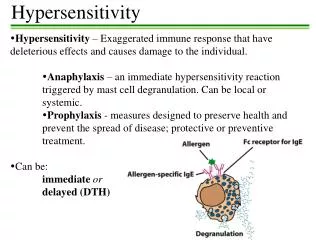
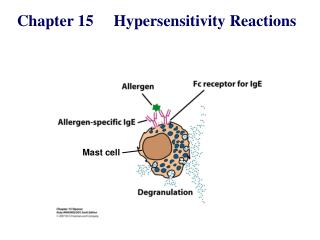
IgE is linked to common allergies Initial exposure -- “sensitization” Humoral response and IgE production Later exposure -- antigen binds to IgE -- mast cell degranulation later Hypersensitivities
Early phase responses Molecular Mediators: Primary– in granules -- histamine -- serotonins, etc. Secondary– synthesized later (w/in 1- few minutes) Localized clinical response (Atopy) atopic asthma: urticaria (hives) eczema (skin lesions) atopic rhinitis food allergies Systemic clinical response (anaphylaxis) anaphylatic shock Hypersensitivities
Late phase responses -- 4-6 hours later e.g., Erythema, etc “peak flow rate” measurements Due to: -- Cytokines from mast cells -- Recruited eosinophils & TH2 -- degranulation Chronic Type I -- eosinophilia -- inflammation: damaged airways & mucous membranes Early phase Late phase Hypersensitivities
What factors affect predisposition toward Type I hypersensitivities? Genetic factors Environmental factors Hygiene hypothesis Hypersensitivities
Treatment Skin testing -- carries some risk Drugs therapies -- Theophylline (blocks degranulation) -- antihistamines (block histamine receptors) -- epinephrine (reverses trachael & bronchiole SM and contracts arteriole SM) Desensitization Desensitization Therapy Hypersensitivities
Type II hypersensitivity -- “Cytotoxic” Ig binding to AG on cells -- triggers cell lysis Complement mediated Macrophage mediated Various types of “immunohemolytic anemia” e.g., Blood transfusion incompatibility {see section in chapter 17} Some penicillin rxs -- other drugs Various autoimmune disorders -- multiple sclerosis -- myasthenia gravis RBC being phagocytosed in fetal erythroblastosis 1967 Science 158: cover Hypersensitivities
Type III hypersensitivity • -- “immune complex” • Localized:(Arthus reaction) • -- could result from an insect bite • Ag-Ab complex • Excess AG small complexes • complement activation • 2) mast cell degranulation • 3) neutrophil recruitment • 4) Triggering of inflammation • Systemic: • Serum sickness • Vasculitis C3a, C5a Hypersensity pneumonitis -- Pigeon breeders disease (pigeon feces dust) -- Farmers lung (Actinomycetes) -- Mushroom picker’s… -- Cheese washer’s… -- Chicken plucker’s… -- etc., … disease Adapted from Majno and Joris, 2004, Cells, Tissues and Disease Type III Hyper Hypersensitivities
Type IV hypersensitivity “Delayed-type” -- slow onset ~day(s) (if sensitized) TH1-cell mediated Sensitization phase-- week(s) onset -- TH1 expansion Effector stage– day(s) onset -- TH1 & macrophage activation -- inflammation Latex type IV hypersensitivity Hypersensitivities
Type IV, cont. Contact Dermatis is a different type of allergic response -- T-cell / macrophage -- involves hapten production -- hair sprays, plant toxins, turpentine, etc. Hypersensitivities Latex type IV hypersensitivity
Tuberculosis (see Chapter 14 pp 212-213) -- Persistent Mycobacterium tuberculosis Granuloma (tubercule) formation TH1cells and activated macrophages ‘caseous’ regions extended tissue destruction Hypersensitivities