Download
1 / 53
530 likes | 862 Views
BLOOD PARASITES PLASMODIA/ BABESIA. WINIFREDA U. DE LEON. SPECIES. PLASMODIUM FALCIPARUM PLASMODIUM VIVAX PASMODIUM MALARIAE PLASMODIUM OVALE PLASMODIUM KNOWLESI. ARTHROPOD -BORNE ANOPHELES MOSQUITOES A. MINIMUS FLAVIROSTRIS HABITAT IN MAN – RBC HIGH OXYGEN TENSION

E N D
BLOOD PARASITESPLASMODIA/ BABESIA WINIFREDA U. DELEON
SPECIES PLASMODIUM FALCIPARUM PLASMODIUM VIVAX PASMODIUM MALARIAE PLASMODIUM OVALE PLASMODIUM KNOWLESI
ARTHROPOD -BORNE ANOPHELES MOSQUITOES A. MINIMUS FLAVIROSTRIS HABITAT IN MAN – RBC HIGH OXYGEN TENSION COMPONENTS: NUCLEUS (CHROMATIN) CYTOPLASM
ON THE MOSQUITO VECTOR NIGHT BITER SLOW FLOWING CLEAN STREAMS FOOTHILLS EXOPHAGIC ZOOPHILIC
LIFE CYCLE SCHIZOGONY ASEXUAL MULTIPLICATION END PRODUCTS – SCHIZONTS (MEROZOITES) OCCURS IN MAN GAMETOGONY GAMETOCYTES OCCURS IN MAN SPOROGONY SEXUAL MULTIPLICATION END PRODUCTS – OOCYSTS (SPOROZOITES) OCCURS IN MOSQUITOES
ASEXUAL STAGES TROPHOZOITES YOUNGEST - RINGFORMS DEVELOPING MATURE SCHIZONTS EARLY DEVELOPING MATURE - MEROZOITES
RED CELL DEFENSES CELL MEMBRANE DUFFY Ag NULL – RESISTANCE TO P. VIVAX HEMOGLOBIN -HEMOGLOBIN S (SICKLE TRAIT) HELPS IN THE SURVIVAL OF PATIENTS FROM P. FALCIPARUM PRIMARY ACUTE ATTACK -B-THALLASEMIA- IMBALANCED GLOBIN CHAIN PROD’N OXIDATION BY HEMICHROMES (REACTIVE O2) G6PD PREVENTS OXIDATION OF THE HEME GROUP DEFICIENCY – GENERATION OF REACTIVE O2 ACCUMULATES IN THE RBC DAMAGES P. FALCIPARUM
VIRULENCE FACTORS RUPTURE OF SCHIZONTS RELEASE OF MEROZOITES: MONOCYTES – TNF (PYROGENIC) OTHER CYTOKINES GLYCOSYLPHOSPHATIDYL INOSITOL (GPI) KNOBS – CYTOADHESION(PfEMP) HISTIDINE RICH PROTEIN (HRP)
MULTI-ORGAN INVOLVEMENT GASTRO-INTESTINAL DIARRHEA, ABD PAIN, NAUSEA, VOMITING, ANOREXIA RESPIRATORY DYSPNEA NON PRODUCTIVE COUGH
FEVER PERIODICITY COINCIDES WITH RUPTURE OF SCHIZONTS INITIAL INFECTION – ASYNCHRONOUS AFTER 5- 7 D - SYNCHRONOUS PF – EVERY 40 HOURS PV & PO - EVERY 48 HOURS PM - EVERY 72 HOURS
PATHO-PHYSIOLOGY DESTRUCTION OF RED BLOOD CELL (INFECTED/ UNINFECTED) PRODUCTION OF CYTOKINES - TUMOR NECROTIC FACTOR (TNF) FEVER, HYPOGLYCEMIA, ARDS SEQUESTRATION IN DEEP VASCULATURE OF INTERNAL ORGANS (RBC RECEPTORS) - INTRACELLULAR ADHESION - VASCULAR ADHESION
HEMATOLOGIC CHANGES ANEMIA LEUKOPENIA THROMBOCYTOPENIA SUPPRESSED HEMATOPOIESIS RETICULOCYTES REDUCED SERUM IRON DEFECTIVE BLOOD CELL MATURATION
PATHO-PHYSIOLOGYSEVERE MALARIA HYPOGLYCEMIA LOW SERUM SODIUM MALABSORPTION (FATS, XYLOSE, VIT B 12 PULMONARY EDEMA CNS DYSFUNCTION ( COMA) ELEVATED BUN, CREATININE, PROTEINURIA
MALARIA OCCURS IN TROPICAL/ SUBTROPICAL COUNTRIES 300-500 M CASES ANNUALLY 1.5.-2.7 M DEATHS 10 LEADING CAUSES OF MORTALITY
MALARIA FIRST FEW DAYS: STEADY LOW GRADE FEVER HEADACHE PHOTOPHOBIA MYALGIA ANOREXIA NAUSEA/ VOMITING
REGULAR CYCLE CLASSIC: CHILLS FEVER SWEATING SPLENOMEGALY ANEMIA JAUNDICE
CAUSES OF ANEMIA HEMOLYSIS SPENIC REMOVAL OF RBC FROM CIRCULATION AUTO-IMMUNE LYSIS DECRASED INCORPORATION OF IRON INTO HEME BONE MARROW DEPRESSION
MALARIA - PHILIPPINES 65-70% P. FALCIPARUM – MALIGNANT 30% P. VIVAX – BENIGN TERTIAN 1% P. MALARIAE - QUARTAN
FALCIPARUM MALARIA INVADES ALL AGES OF RBC SEQUESTRATION IN INTERNALORGANS ISCHEMIA LIVER – ABDOMINAL PAINS JAUNDICE LUNGS – PULMONARY EDEMA KIDNEYS - BLACKWATER FEVER- HEMOGLOBINURIA CEREBRAL INVOLVEMENT
COMPLICATED COMA CONVULSIONS HYPOGLYCEMIA ACIDOSIS RESPIRATORY DISTRESS ALGID (CIRCULATORY COLLAPSE, SHOCK & SEPTICEMIA) HYPER-PARASITEMIA
VIVAX MALARIA LESS SEVERE RELAPSES OCCUR AFTER WEEKS OR MONTHS INVADES ONLY RETICULOCYTES LOW ALBUMIN/ ELEVATED GLOBULIN INCREASED SERUM POTASSIUM
MALARIAE MALARIA INVADES OLDER RBC LONGER INCUBATION PERIOD NEPHROTIC SYNDROME – DEPOSITION OF IMMUNE COMPLEXES LATENT INFECTION FOR MANY YEARS
WHO ARE AT RISK? THOSE IN ENDEMIC PLACES CHILDREN PREGNANT WOMEN SPONTANEOUS ABORTION CONGENITAL INFECTIONS LOW BIRTH WEIGHT PRE-TERM DELIVERY PERI-NATAL DEATH TRAVELERS BLOOD RECIPIENTS- TRANSFUSION
PHILIPPINES 14.8% AT RISK SOLDIERS FARMERS INDIGENOUS CULTURAL GROUPS MINERS FOREST WORKERS 65/ 79 PROVINCES 8TH LEADING CAUSE OF MORBIDITY
MALARIA FREE AKLAN GUIMARAS BILIRAN ILOILO BOHOL LEYTE CAMIGUIN LEYTE DEL SUR CAPIZ N/ SAMAR CATANDUANES SIQUIJOR CEBU
HIGHLY ENDEMIC PLACES PALAWAN KALINGA-APAYAO IFUGAO AGUSAN DEL SUR
DIAGNOSIS CLINICAL – MIMIC DISEASE GASTROENTERITIS PNEUMONIA MENINGITIS HEPATITIS ENCEPHALITIS DENGUE TYPHOID TRAVEL Hx
LABORATORY Dx BLOOD SMEARS THICK/ THIN STAIN WITH WRIGHT’S OR GIEMSA FLOURESCENT STAINING (QBC) SEROLOGY: ANTIBODY DETECTION: IFAT ELISA ANTIGEN DETECTION : RAPID DIAGNOSTIC TESTS (RDT’S) HRP II LDH PCR
TREATMENT NON FALCAPARUM: CHLOROQUINE ORAL UNCOMPLICATED FALCIPARUM CHLOROQUINE ORAL QUININE ORAL FANSIDAR (SULFADOXINE PYREMETHAMINE) PRIMAQUINE – HYPNOZOITES/ GAMETOCYTES CHECK FOR G6PD DEFICIENCY ARTEMISININ (QINGHAOSU) CO-ARTEM COMPLICATED MALARIA – HOSPITALIZE (IV MEDICATION) PROPHYLAXIS – CHLOROQUINE PROGUANIL
PREVENTION • Mosquito nets • Clean clothing
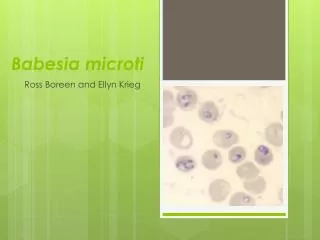
BABESIA- PIROPLASMA BLOOD PARASITES THAT CAUSES HEMOLYSIS B. MICROTI - USA B. DIVERGENS - EUROPE TICK-BORNE – IXODES spp LYME DISEASE BLOOD TRANSFUSION
BABESIOSIS -PIROPLASMOSIS MANIFESTATIONS IRREGULAR FEVERS CHILLS SWEATING PAIN/ MALAISE LETHARGY SEVERE CASES HEMOLYTIC ANEMIA JAUNDICE SHORTNESS OF BREATH HEMOGLOBINURIA