Download
1 / 16
450 likes | 2.16k Views
Transverse Myelitis. Emily O. Jenkins MD, PGY3 AM Report 12.18.09. Transverse Myelitis (TM) . Immune-mediated process results in neural injury to the spinal cord Varying degrees of weakness, sensory alterations and autonomic dysfunction

E N D
Transverse Myelitis Emily O. Jenkins MD, PGY3 AM Report 12.18.09
Transverse Myelitis (TM) • Immune-mediated process results in neural injury to the spinal cord • Varying degrees of weakness, sensory alterations and autonomic dysfunction • Up to half of idiopathic cases will have a preceding respiratory or gastrointestinal illness
Spectrum of Neuroimmunologic Disorders Acute inflammatory demyelinatingpolyneuropathy 2. Chronic inflammatory demyelinatingpolyneuropathy 3. Acute disseminated encephalomyelitis 4. pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections
TM: Incidence • Rare: Estimated between 1 and 8 cases per million people per year • 1400 new cases reported in US each year • Affects individuals of all ages with a bimodal peak between ages 10-19 and 30-39
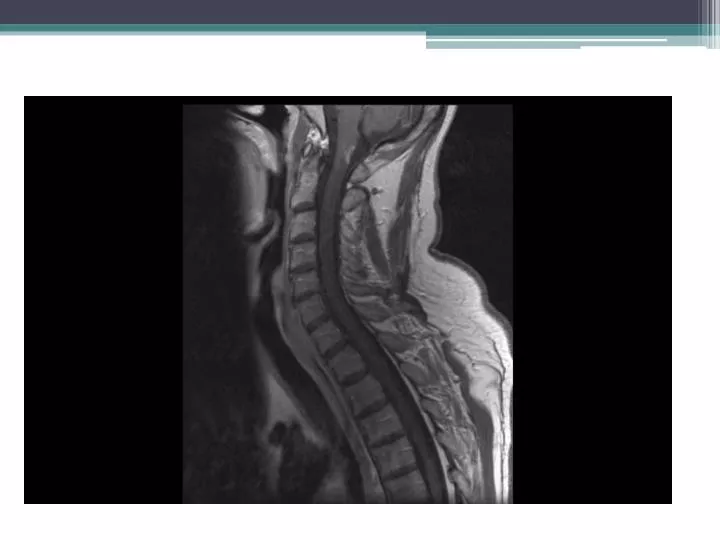
Presentation • 50% will lose all movement in legs • Nearly all have some degree of bladder dysfunction • 80-94% have numbness, paresthesias, or band-like dysethesias • Autonomic symptoms may include: urgency, incontinence, difficulty or inability to void, incomplete evacuation of bowel and/or bladder, sexual dysfunction • 80% of patients reach clinical nadir within 10 days of symptom onset • Thoracic spinal cord most typically involved in adults, cervical spinal cord in children
Alternative diagnostic considerations • B12 deficiency: slowly progressive weakness, sensory ataxia, paresthesias • Radiation myelopathy • Hepatic myelopathy: rare neurologic complication of chronic liver disease with portal hypertension • Decompression sickness: complication of deep sea diving • Neurolathyrism: prolonged consumption of grass or chickling pea; slowly developing paraparesis with paresthesias; no treatment • Konzo: acute spastic paraparesis from high exposure to cyanogenic compounds in diets containing insufficiently processed bitter cassava
Etiology • Acquired alteration in the innate or acquired immune system • Cellular injury and dysfunction • Infectious trigger: infectious agent triggers breakdown of immune tolerance for self-antigens • TM and ADEM: Superantigen-mediated activation of T lymphocytes • Suspected that multiple immune system components contribute to observed dysfunction including T and B lymphocytes, macrophages, and NK cells • Mechanism of injury also probably involves multiple pathways including T lymphocyte killing of neural cells, cytokine injury, activation of toxic microglial pathways, immune-complex deposition, and apoptosis
TM and MS • TM can be the presenting feature of MS • Patients ultimately diagnosed with MS are more likely to have: • asymmetric clinical findings • predominant sensory symptoms with relative motor sparing • MRI findings extending over fewer than two spinal segments • abnormal brain MRI • oligoclonal bands
Treatment • No consensus guidelines • Mainstays include: • corticosteroids: no randomized trials • plasmapheresis: moderate to severe cases, or those who do not respond to steroids after 3-5 days • Pulse dose IV cyclophosphamide • CSF filtration therapy: spinal fluid is filtered for inflammatory factors (not available in US) • For severe, refractory cases: 2 year course of azothioprine, methotrexate, mycophenolate, or oral cyclophosphamide
Prognosis • Most will have monophasic disease • Up to 20% will have recurrent inflammatory episodes within the spinal cord • Significant recovery is unlikely if no improvement by 3 months
Recurrence • Predictors of recurrence: • Multifocal lesions within the spinal cord • Demyelinating brain lesions • CSF oligoclonal bands • Mixed connective tissue disorder • SS-A antibodies • Persistently high IL-6 levels in CSF: thought to lead to high NO production and subsequent neural injury • Predictors of poor outcome: • Initial complaint of back pain • Rapid progression to maximal symptoms within hours of onset • Spinal shock • 14-3-3 protein, a marker of neuronal injury, in CSF during acute phase