Download
1 / 20
200 likes | 457 Views
Case 26: 25 y.o. Male. Right shoulder. Keloid? Hypertrophic scar? Lichen simplex chronicus?. On Examination Approximately 5x4cm dermal nodule Firm texture right shoulder no lymphadenopathy. On examination.

E N D
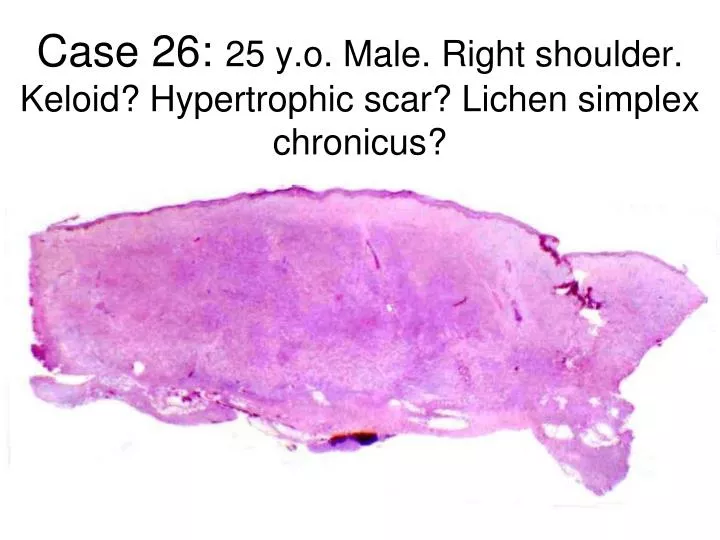
Case 26: 25 y.o. Male. Right shoulder. Keloid? Hypertrophic scar? Lichen simplex chronicus?
On Examination Approximately 5x4cm dermal nodule Firm texture right shoulder no lymphadenopathy. On examination The initial impression was this was a cyst and excision was organised by his GP on a General Surgery Minor ops list.
Histopathology • Unencapsulated spindle cell lesion • composed of short fascicular arrays in a storiform pattern • nestled within the mid-dermis extending widely into sub-cutis. • Scattered melanophages were noted. Immunolabelling showed strong positivity for CD34 and very focal nonspecific positivity for SMA & Factor XIIIa
CD34 S100
CASE 26 • A.Hypertrophic scar • B. Fibroma • C. Perineuroma • D. Dermatofibrosarcoma • E. Dermatomyofibroma
CASE 26 • A.Hypertrophic scar • B. Fibroma • C. Perineuroma • D. Dermatofibrosarcoma • E. Dermatomyofibroma Features consistent with a pigmented dermatofibrosarcoma protuberans or Bednar tumour.
Bednar Tumour Pigmented DFSP varies from ordinary DFSP by the presence of non neoplastic melanin- laden dendritic cells; it is otherwise morphologically and clinically identical to ordinary DFSP Czech pathologist, Blahoslav Bednar (1916- 1998), first described the Pigmented DFSP in 1957 while describing a group of cutaneous tumours demonstrating prominent storiform pattern and melanin pigment which were thought to be a variant of Neurofibroma. Less than 5% of dermatofibrosarcoma protuberans (DFSP) tumours are pigmented.
Dermatofibrosarcoma Protuberans • Rare- 1 case per million per year • Cutaneous soft tissue sarcoma originating from Fibroblasts • 90% are low grade, 10% contain an additional high grade sarcomatous component therefore it is considered to be of intermediate malignancy • <4% of tumours can metastasise/transform fibrosarcomatous • Peak incidence is adults in third decade
Pathophysiology • 90% of DFSP have the translocation between Ch17 and Ch22 [t(17:22)] • Creates a fusion between a collagen gene and platelet derived growth • Resultant fusion gene creates platelet derived growth factor (PDGF) • Fibroblasts carry the platelet-derived growth factor receptor β • Malignant cells produce PDGF which stimulates fibroblast growth • As malignant cells develop, tumour enlarges
Mortality/morbidity • locally aggressive with high recurrence rate • 5-year survival - 99.2% • metastasis rare (only 1-4% reported)
Prognosis & Adjunct Therapy • Tumour depth is the only factor associated with disease- free survival • Follow-up should involve • Metastatic/ unresectable tumours can be treated with Imatinib mesylate (Glivec) if t(17:22) positive • There is a role for radiotherapy after surgery
BB was referred to the Skin Cancer MDT for further management On examination, he had his original scar on the right shoulder as well as remnants of his DFSP Management
Medical Treatment • Radiation therapy • margins positive • Postoperative – reduce risk of recurrence
Wide Local Excision Mohs Surgery Excision Vs. Goal is achieve clear surgical margins with some form of complete circumferential and peripheral deep margin assessment before reconstruction
Management of DFSP Matin, R.N., Acland, K.M. and Williams, H.C. (2012) British Journal of Dermatology, 167: 6–9. No randomized controlled trials exist, probably due to the rarity and varied presentation of DFSP. A recent published review of the literature highlighted that evidence for superiority of either procedure was limited.
Medical Treatment • Imatinib • inhibitor protein-tyrosine kinases • platelet-derived growth factor (PDGF) receptors • unresectable, recurrent, metastatic DFSP • preoperative therapy • decrease tumour load • promote tumour cell apoptosis • reduce the extent of surgery.