Download
1 / 117
1.22k likes | 2.01k Views
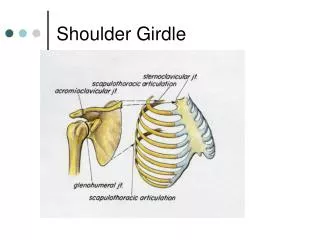
Shoulder Girdle Pathology. Shoulder Pain:. Fractures of the shoulder girdle complex. Clavicle: 75% occur in children under 13 Proximal fracture Rare, differentiate from epiphyseal injuries Middle Third fracture- Most common, 80%

E N D
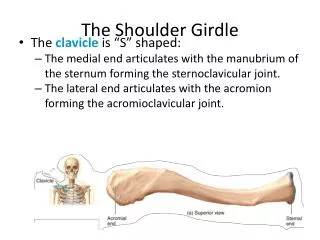
Fractures of the shoulder girdle complex Clavicle:75% occur in children under 13 • Proximal fracture • Rare, differentiate from epiphyseal injuries • Middle Third fracture- Most common, 80% • Usually displaced upward by pull of the sternocleidomastoid muscle • Distal fracture • Displaced downward by the weight of the arm.
MOI: • Fall on the lateral aspect of the shoulder • Fall on outstretched arm (FOOSH)
RX: Arm sling For the first 1-2 weeks To support the weight of the arm. Figure of eight Figure of eight bandage, intent is to reduce the motion at the fracture site. Worn for a period of at least 6 weeks (adults) or 4 weeks (child). Can use the arm as wanted & symptoms allow.
Scapular Fractures • 1% of all fractures • High energy: fall or direct blow • Associated Injuries • Ipsilateral rib fractures • Pulmonary trauma • Clavicular fractures • Brachial plexus injuries • Subclavian artery injuries • Classified according to location
Scapula: Type I: fractures of scapular body 2 Type II: fractures of apophyseal regions including acromion and coracoid process3,4 Type III: fracture of superolateral angle including glenoid neck and fossa1 RX: generally minimal treatment. Surgery only in most drastic, displaced fractures. Donatelli RA, 1987
Scapular Fractures requiring surgery Acromion or scapular spine fractures with a doward tilting of the lateral fragment and subacromial narrowing Coracoid fractures that extend into the glenoid fossa Glenoid rim and intra-articular glenoid fractures associated with glenohumeral instability
Rx of Scapular Fractures Sling 7-10 days Progressive regimen of pendulum and gentle ROM exercises Progressive AROM and strengthening exercises
Humeral Head Fractures Fracture Dislocations
Proximal: A. Greater Tuberosity More commonly seen in older individuals. B. Lesser Tuberosity Rare, usually avulsion fractures C. Neck of the Humerus Common fractures, transverse, comminuted, impacted D. Shaft of the Humerus MOI: significant force applied directly or indirectly to shoulder region Rx: depends upon the type of fracture, age of the patient
Fractures Associated with Shoulder Dislocations Hill-Sachs lesion: • depression fracture of the posterior/lateral humeral head. • Area of soft cancellous bone which is compressed against the glenoid rim. • Occurs in 77% of traumatic anterior dislocations http://www.athleticadvisor.com/Injuries/UE/Shoulder/shoulder_dislocation.htm
Bankart Lesion www.sportsortho.co.uk/article.asp?article=86 • Defined as a detachment of the labrum from the glenoid rim, on the anterior • occur in 87% of the traumatic dislocations • the most common reason for recurrent instabilities • Increase rate of reinjury
Quality of the Tissue • Good tissue quality: heal faster, less functional issues • Poor tissue quality: will the repair hold, takes longer to heal, more functional deficits after surgery • Specifics of the Case: • Did it involve the Biceps Tendon or not? • Removal of any bone? • Other?
Osteonecrosis • Snowcap is one of the first signs of osteonecrosis. • Compression will hurt more as the blood supply is cut off more.
Rotator Cuff Dysfunction Resulting in Impingement • Key pathophysiological factors • Primary or secondary impingement • Tensile overload • Macrotraumatic tendon failure • Posterior or undersurface impingement • Key Muscles and Force Couples • Deltoid Rotator cuff force couple • Deltoid force: Supraspinatus initiator, then deltoid. Therefore if supraspinatus torn, then the shoulder will go straight upand cause impingement. So t(x) will be using other RC to stabilize and how to pull down the humeral head. • Rotator Cuff force: • Trapezius and Serratus anterior • Anterior posterior rotator cuff force couple • Concavity-compression mechanism
Rotator Cuff Impingement • Primary Compressive Disease: Primary Impingement • Compression of rotator cuff tendons between the humeral head and the overlying anterior third of the acromion, coracoacromial ligament, coracoid or AC joint • Subacromial space • Normals: 6mm-14mm • Patients with shoulder pain: 7mm-13mm
Neer Classification Stage I: characterized by edema, inflammation, hemorrhage in the subacromial space. Swelling is responsible for the impingement • Risk Factors: age 25 or less • SX: dull ache in the shoulder after activity, pain may interfere with ADL’s • Start of the cascade
Signs: painful arc in abduction - between 60 and 120 dg, pain free • PROM, resisted tests are strong but painful for abduction • Palpation: tender over the greater tuberosity and the anterior edge of the acromian • Special tests: + Neer impingement test, + Kennedy and Hawkins test. • This stage is easy to reverse if the person rests from aggravating activities and changes some work or play postures, strengthens weak muscles • AROM painful arch is always present, but not during passive.
Stage II: Characterized by aggravation of the subacromial contents creating a thickness in the bursae and fibrosis of the tendons. • Risk Factors: 25 to 40 years of age • SX and Signs: similar but increased in intensity from Stage I • Impairments: more limitation in the PROM and with Hawkins and Kennedy test there is a catching sensation with the return from an elevated position. • More difficult to reverse than Stage I
Stage III: More complicated: • get a partial or full thickness tendon tear, • changes in the bony configuration of the humeral head and acromion, • osteophytes • Risk Factor: 40 years of age or greater • SX: increase in intensity of symptoms, interferes with daily activities • Signs: AROM more limited than PROM, resisted tests show weakness in abduction and external rotation
X-Rays: cystic changes in the greater tuberosity, underside of the acromian or at the AC joint RX: surgery if conservative treatment doesn’t work. Repair of the torn muscles would occur with all of the surgical options. Surgical Options: 1. coracoacromial ligament resection 2. anterior acromioplasty 3. distal clavicle resection (Mumford procedure) 4. AC joint inferior osteophyte resection
Mechanical Impingement: • Abnormal shape of the acromion. • 3 types of acromion, flat, curved and hooked. • There is a close association with a hooked acromion (70%) with full thickness rotator cuff tears; 80% association with impingement syndrome
Secondary Compressive Disease • Due to underlying instability of the GH joint • Anterior instability – overhead athletes, throwing athletes • Increase in anterior translation, biceps tendon and rotator cuff become impinged • Continual loss of GH stability • Leads to rotator cuff tears • Usually supraspinatus
Tensile Overload • Repetitive intrinsic tension overload • Occurs during deceleration and follow through • High load placed on posterior rotator cuff muscles • Pathological changes of angiofibroblastic hyperplasia – early tendon stages, progresses to tears • Tendinosis injuries • Degenerative process
Macro traumatic Tendon Failure • Single traumatic event or a previous traumatic event • Forces are greater than the tendon can handle • Normal tendons don’t tear • 30% damaged to produce a substantial reduction in strength • Full thickness tears • Bony avulsions • May have had repeated microtraumatic insults and degeneration over time • Failure over one heavy load
Posterior impingement • Undersurface • In 90 dg of abduction and 90 dg of Ext rotation • Supraspinatus tendon and infraspinatus tendon rotate posteriorly and get pinched between the humeral head and the posterior-superior glenoid rim
Add anterior translation of the humeral head causes mechanical fraying on undersurface of the rotator cuff tendons • Halbrecht et al studied baseball pitchers with MRI of shoulder • Paley et al studied 41 professional throwing athletes – all had this problem
Rotator Cuff Pathology • Best management of a tear depends upon: • Size and duration of the tear, age of the tear, force that caused the tear. Massive tear of Supraspinatus tendon
Rotator Cuff Pathology Partial Thickness (more common) and can involve the superior aspect, the mid-substance of the muscle and the inferior aspect of the muscle. • Incomplete tear • Superior surface or undersurface of rotator cuff • Superior surface tears: usually result of subacromial impingement • Undersurface tears associated with tensile loads and GH joint instability Full Thickness tears: are pure transverse rupture, pure vertical tear, longitudinal split can occur which parallels the tendon fibers • Entire thickness of muscle is torn • Initiated in critical zone of supraspinatus and can extend into infraspinatus, teres minor and subscapularis
Tear size • Small Tears: < 1cm • Medium Tears: 1-3cm • Large tears: 3-5 cm • Massive tears: > 5 cm, tendon is often retracted • Larger tears are immobilized for longer periods of time • Compete tear patterns: • Crescent – shaped tears, don’t usually retract, repaired directed to greater tuberosity • U-shaped: greatest extent in longitudinal direction to the tendon
HX: age is 40 years or older with previous shoulder symptoms or injuries • Acute tears (no previous shoulder problems) • Occur in 5-8% of all rotator cuff tears • Usually associated with trauma • Younger individuals: tear is a result of repetitive forceful use of arm overhead, • Secondary result from the muscle imbalance, sudden definite injury to the shoulder. • Rupture in a younger patient usually is an avulsion of the tendon from the greater tuberosity rather than a tear within the muscle itself
Supraspinatus Muscle • Muscle most likely to be implicated in a rotator cuff tear. • 90% are due to structural impingement on the supraspinatus from the overlying coracoacromial arch. HX: attritional or degenerative tear Most occur in the posterior region, area near the junction of the supraspinatus and infraspinatus 13-17 mm posterior to biceps tendon Acute injury: FOOSH, abduction movement with a high force and velocity
SX: • pain in the lateral aspect of the arm • may radiate in the region of the biceps • rarely below the elbow • night pain • can’t sleep on the shoulder, • complaints of shoulder weakness
Signs: • Observation: difficulty elevating arm • AROM: decreased ROM particularly in abduction PROM: not significantly limited unless a chronic condition or a very painful, acute injury • Resisted tests: ABD/ER weakness • Palpation: tenderness at the insertion of the muscle at the greater tuberosity or in the muscle belly http://www.youtube.com/watch?v=gvhfiuGrESQ
Surgery: Basic Information • Repair: try to mimic the supraspinatus footprint width but not necessarily the size of the original insertion • Type of Surgery: • Open • Mini • Scope • Other • Type of Fixation • Anchor? • Placed at 45 dg angle to resist pull out • Sutures? How were they used – single row, double row • Mattress stitch, simple or combination • Staples – no longer in use http://www.youtube.com/watch?v=Ch2FnzIW7QE&feature=related
Myofascial Dysfunction of the Shoulder Girdle Chronic shoulder girdle pain or dysfunction HX: progressive spread of pain, exacerbations, remissions which are related to activity. Usually affects only one area rather than several as with fibromyalgia. SX: muscle point tenderness, pain with activity, better with rest
Signs: absence of joint signs overall decrease in ROM but minimal at first PROM will equal AROM Swelling over the muscle Crepitus in the muscle Trigger points in the muscle Radiographs, neurological tests and imaging studies are all normal RX: correct muscle imbalances, trigger point stretch/spray techniques, pain relief, posture instruct
Tendonitis • Supraspinatus Tendonosis • Long head of the biceps tendinosis • Calcific tendonitis
Musculotendinous Dysfunctions of the Glenohumeral Joint TendonitisRotator Cuff Tendonitis: inflammation of any of the four rotator cuff muscles, most common is the supraspinatus tendon HX: overuse syndrome, occurs most often with overhead activities
SX: acute: severe pain, not well localized chronic: low-grade aching, • fatigue sensation, localized to the lateral aspect of the upper arm or deltoid • difficulty sleeping on the Arm, • catching sensation with the arm in flexion or internal rotation
Signs: • AROM: pain with active abduction, external rotation painful arc: 70 to 120 dg elevation • PROM: full, painfree except in acute stages where there may be pain due to swelling and causing an impingement • chronic: IR/ER may be slightly limited with pain
Resisted Tests: Supraspinatus: weak and painful. Pain without weakness: more acute tendonitis Pain with weakness: partial tear in the tendon • Special tests: • Neer + impingement test • Hawkins and Kennedy + impingement test • Supraspinatus test: empty can test • + Lift off test indicates subscapularis
RX: • Conservative at first, may use anti-inflammatory medication • PT: cross friction massage over the tendon, modality use, look at body mechanics and muscular imbalances to help decrease strain on the tendon.
Physician treatment or surgery • Arthrogram and MRI are the diagnostic tools, • Surgery will be an acromioplasy, • Release of acoacromial ligament or a bursectomy. • Surgery usually occurs with chronic cases only.
Biciptal Tendonitis: second most common site of tendonitis in the shoulder. Affects the intra-articular portion or close to the site of its origin as it passes through the bicipital groove, or at the groove. Intra-articularbicipital tendonitis with supraspinatus tendonitis cn occur. In the groove, the biceps tendon can sublux and causes fraying and swelling of the fibers and the tendon sheath
Causes: eccentric over loading due to deceleration of the elbow repeated elbow extension repetitive overhead use HX: no specific history, repetitive overhead activities, occasionally a single event or trauma will cause the problem
SX: pain with activity, decreases with rest, initially can be quite painful and will later decrease overall Signs: AROM and PROM show normal range with only a slight limitation of range in passive ROM abduction and IR are limited secondary to pain Resisted tests: shoulder flexion, elbow flexion, supination will all be painful, can be strong or weak depending on the condition of the tendon Palpation: tender over the bicipital groove
Special tests: speed’s test is + Yergason’s test is + RX: initially is conservatively with PT Physician: corticosteroid injection, surgical: decompression of the acromial arch, excision of the transverse humeral ligament
Calcific Tendonitis • Deposition of calcium into the tendon • most common tendon is the superspinatus • Found in the avascular portion of the tendon. • Deposits may be a result of pressure at the avascular region or with a decrease in the O2 supply. • Tenocytes transform into chondrocytes and lay down calcium deposits • Self Healing: has cycles of deposition and absorption