Download
1 / 8
210 likes | 1.5k Views
1. Diagnostic approach to pleural effusion. The history and physical examination are critical in guiding the evaluation of pleural effusion. Chest examination of a patient with pleural effusion

E N D
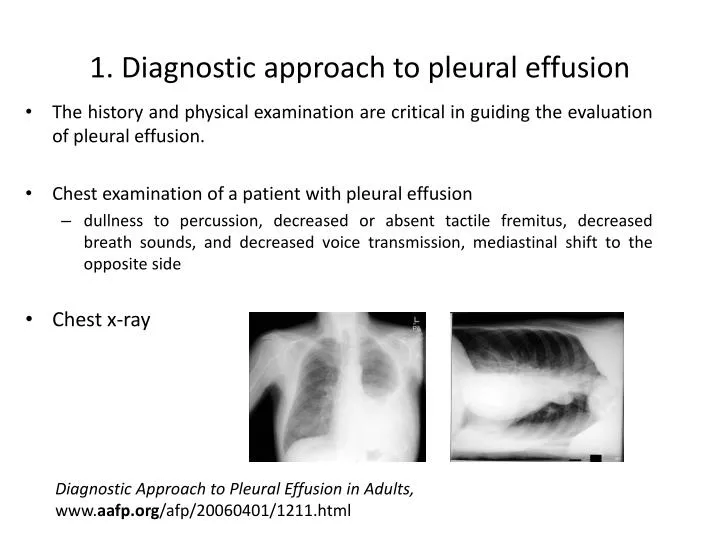
1. Diagnostic approach to pleural effusion • The history and physical examination are critical in guiding the evaluation of pleural effusion. • Chest examination of a patient with pleural effusion • dullness to percussion, decreased or absent tactile fremitus, decreased breath sounds, and decreased voice transmission, mediastinal shift to the opposite side • Chest x-ray Diagnostic Approach to Pleural Effusion in Adults, www.aafp.org/afp/20060401/1211.html
Diagnostic approach to pleural effusion • The first step in the evaluation of patients with pleural effusion is to determine whether the effusion is a transudate or an exudate. Harrison’s Internal Medicine 17th edition p.1658
Diagnostic approach to pleural effusion • Transudative and exudative pleural effusions are distinguished by measuring the lactate dehydrogenase (LDH) and protein levels in the pleural fluid. • Thoracentesis • invasive procedure to remove fluid or air from the pleural space for diagnostic or therapeutic purposes Harrison’s Internal Medicine 17th edition p.1658
Diagnostic approach to pleural effusion • Perform diagnostic thoracentesis: • if the etiology of the effusion is unclear • if the presumed cause of the effusion does not respond to therapy as expected. • Pleural effusions do not require thoracentesis: • if they are too small to safely aspirate (<1 cm thickness on a lateral decubitus film) • if their presence can be explained by underlying congestive heart failure, etc. http://emedicine.medscape.com/article/299959-diagnosis
Diagnostic approach to pleural effusion Light’s criteria • Exudative pleural effusions meet at least one of the following criteria, whereas transudative pleural effusions meet none: 1. pleural fluid protein/serum protein >0.5 2. pleural fluid LDH/serum LDH >0.6 3. pleural fluid LDH more than two-thirds normal upper limit for serum Harrison’s Internal Medicine 17th edition p.1658
Diagnostic approach to pleural effusion • The criteria misidentify ~25% of transudates as exudates. If one or more of the exudative criteria are met and the patient is clinically thought to have a condition producing a transudative effusion, the difference between the protein levels in the serum and the pleural fluid should be measured. • If this gradient is greater than 31 g/L (3.1 g/dL), the exudative categorization by the criteria can be ignored because almost all such patients have a transudative pleural effusion. Harrison’s Internal Medicine 17th edition p. 1658
Diagnostic approach to pleural effusion • The primary reason to make this differentiation is that additional diagnostic procedures are indicated with exudative effusions to define the cause of the local disease. • If a patient has an exudative pleural effusion, the following tests on the pleural fluid should be obtained: • description of the fluid • glucose level • differential cell count • microbiologic studies • cytology Harrison’s Internal Medicine 17th edition p. 1658