Download
1 / 72
810 likes | 1.54k Views
Malignant Pleural Effusion: Prevalence. ~ 200,000 MPE / year in USA 1:4 Lung Cancer pt; 1:3 Breast; 9:10 Mesothelioma ~ 100,000 MPE from Lung Cancer / yr in Europe Pleural effusion is the first sign of cancer in 25% of patients with MPE.

E N D
Malignant Pleural Effusion: Prevalence • ~ 200,000 MPE / year in USA 1:4 Lung Cancer pt; 1:3 Breast; 9:10 Mesothelioma • ~ 100,000 MPE from Lung Cancer / yr in Europe • Pleural effusion is the first sign of cancer in 25% of patients with MPE Light RW & Lee YCG. Textbook of Pleural Disease, 2nd ed. 2008
Malignant Pleural Effusions • 95% MPM pts suffer from a pleural effusion • Dyspnea most common presenting symptom • Fear of ‘drowning to death’
Malignant Effusion: significant burden Western Australia (population 2 million): ~8,000 inpatient bed days per year US$10 million inpatient cost per year
Myths in Malignant Effusions Although MPE common recent advances in knowledge has shed light on many myths in • Why symptoms develop • Diagnostic workup and limitations • Pleurodesis and its limitations • Indwelling pleural catheters: pros and cons
Myth: Patients with malignant effusions are breathless because the fluid compresses on the lung, restricting its expansion.
Why are patients breathless? Effects on Lung Function:For 1 L fluid drained: FEV1 or FVC 0.2 L; TLC 0.4 L Lung Compression not the key factor • Effects on Diaphragm: • Weight of the effusion profoundly affects the diaphragm • Dyspnea related to effect on the diaphragm: - No dyspnea if diaphragm domed and moves normally - Severe dyspnea if diaphragm inverted and not move with respiration Lee YCG & Light RW. in Encyclopedia of Respiratory Disease 2006
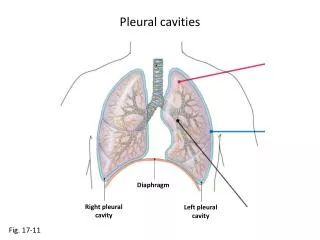
Why are patients breathless? The pleural cavity expands to accommodate the fluid. Altered respiratory mechanics contribute to breathlessness
Why are patients breathless? Drainage of effusion remove weight from hemidiaphragm and restore respiratory mechanics
Large effusion Diaphragm inverted Small effusion Diaphragm normal Courtesy: Dr Naj Rahman
3L effusion 3kg Sofia Lee born Sept 09 2.93kg
Myth: Drainage of effusion in patients with a trapped lung is not useful.
Drainage of effusion in patients with a trapped lung can still improve symptoms 70/M Metastatic Thyroid Cancer
Myth: The more fluid sent for cytology, the more likely you can make a malignant diagnosis.
Pleural fluid for Cytology Analyses ‘More likely to make a malignant diagnosis on cytology if you send more fluid?’ True or False No significant increase in sensitivity of cytology when >50mL of fluid is sent: Swiderek J et al Chest 2010 Abouzgheib W et al Chest 2009 Sallach SM et al Chest 2002 Anderson CB et al Cancer 1974
Benign MPM TTF-1 Indication: Diagnosis of Pleural Malignancy Cytology diagnostic sensitivity 20-60% depends on: type of tumor (adeno >> mesothelioma) experience of cytologists tumor load Light RW & Lee YCG. Textbook of Pleural Disease, 2nd ed. 2008
Myth: Pleuroscopy or Thoracoscopy biopsy can safely exclude malignant pleural disease.
Pleuroscopy / Medical Thoracoscopy Jacobaeus performing thoracoscopy Felice Cova Tassi GF. International Pleural Newsletter 2004
Thoracoscopy is not gold standard • 142 Medical Thoracoscopy / Pleuroscopy • Negative Predictive Value 90% • False negative occurs – all mesothelioma • Similar rate to previous papers • - despite advances in immunohist/thoracoscopy
Mesothelioma: diffuse thickeningbiopsy often fibrous tissue onlyfalse negative possible
Myth: FDG PET is not useful in management of malignant pleural diseases.
PET • Limited diagnostic value: • Malignancy vs benign pleural diseases • Mesothelioma vs metastatic carcinoma West SD & Lee YCG. Clin Pulm Med 2006
Percutaneous biopsy guided by PET/CT Evolving option. In selected patients can be useful.
Semiquantitative FDG PET using volume-based parameter of TGV Prognosis Response – 1 cycle chemo Francis et al J Nucl Med 2007;48:1449-1458 Nowak et al. Clin Cancer Res; 2010, 16(8); 2409–17.
FLT – Fluorothymidine Thymidine is a pyrimidine analogue incorporated into DNA CELL PROLIFERATION tracer Not influenced by pleural inflammation, infection or pleurodesis Novel Tracers in mesothelioma Courtesy Prof Ros Francis (Australia)
FLT PET response assessment baseline post chemo Courtesy Prof Ros Francis (Australia)
Hypoxia imaging in mesothelioma FMISO PET-CT FDG PET-CT
18F-Annexin Phase I: apoptosis markerScan before vs after chemotherapy to assess response
Myth: Pleurodesis is the standard first choice for management of malignant pleural effusions.
Pleural Effusion: Management • This approach is now strongly challenged i) Pleurodesis (talc) is less efficacious as often reported and can induce significant complications ii) Aim for management is relief of Dyspnea and QoL: Drainage is the key Light RW & Lee YCG. Textbook of Pleural Diseases 2nd ed 2008
Courtesy Dr Rodriguez Panadero
Controversy: Is talc better delivered via • thoracoscopy (poudrage) or chest tube (slurry) ‘Talc poudrage is superior: Distribute talc over entire pleural surface’ Fact or Myth? Courtesy Dr Carla Lamb
TALC IS NOT GLUE !!! Even spread over pleura not essential
Dresler CM. Chest 2005: Multicenter phase III study talc poudrage (n=242) vs slurry (n=240) at 6 months < 50%
Complications of Talc Pleurodesis Dresler CM. Chest 2005: CALGB phase III study • More side effects from thoracoscopic (VATS) poudrage • 2.3% patients died from ARDS
Talc Pleurodesis Significant shortcomings: • Success rate low (70%) even in selected patients • Unsuitable in trapped lung Overall <50% pts benefit • Side effects common: can be lethal
Do we really need to create pleurodesis? Relieve symptoms without pleurodesis using Ambulatory Small Bore Catheter Drainage
Tunnelled Indwelling Pleural Catheter • Ambulatory drainage outside hospital • Patient controlled drainage whenever breathless
Tunnelled Indwelling Pleural Catheter • 39,000 units sold in USA alone each year • 1st choice for malignant effusion in many centers
Malignant Pleural Effusion Talc Pleurodesis Indwelling Pleural Catheter Cost Economics: Bed days; Inpatient costs
IPC significantly reduce hospital days for patients with malignant effusions over talc pleurodesis Fysh E et al. Chest 2012
Randomized Trial on Management of Malignant Effusion using Indwelling Pleural Catheters(British Lung Foundation) Malignant Pleural Effusions n=110 randomize Ambulatory indwelling catheter drainage Standard care & in-patient talc pleurodesis Visual Analog Score for breathlessness (daily) QoL: Wks 1, 2, 4, 6, 10, 14, 18, 22, 26, 39, 52
Indwelling Pleural Catheters offer the same improvement in QoL as talc pleurodesis From: Effect of an Indwelling Pleural Catheter vs Chest Tube and Talc Pleurodesis for Relieving Dyspnea in Patients With Malignant Pleural Effusion: The TIME2 Randomized Controlled Trial JAMA. 2012;307:2383-9
Cost-Effectiveness • Puri V et al. Ann Thorac Surg.2012 • Treatment of Malignant Pleural Effusion: • A Cost-Effectiveness Analysis • The most cost-effective treatment for a malignant pleural effusion (in USA setting): • Indwelling Pleural Catheter if survival short (3 mths) • Bedside Pleurodesis if survival > 12 mths
Define place of IPC in management algorithm of MPE • Define optimal management and aftercare • Significant potential to grow in its use in both malignant and non-malignant effusions Fysh E and Lee YCG. J Thorac Oncol 2011
Myth: Indwelling pleural catheters are associated with significant and serious complications eg infection, protein loss.
Complications of Indwelling Catheters Wrightson J, Fysh E, Maskell N, Lee YCG. Curr Opin Pulm Med 2010