Download
1 / 15
360 likes | 2.12k Views
Diagnostic Approach to Pleural Effusion. Garrett Waagmeester 4/25/2014. Normal Pleural Physiology. Total pleural fluid volume: 0.2-0.3 mL /kg Fluid produced by systemic vessels of the parietal pleura, primarily less dependent capillaries, based on: Permeability of the pleural vessels

E N D
Diagnostic Approach to Pleural Effusion Garrett Waagmeester 4/25/2014
Normal Pleural Physiology • Total pleural fluid volume: 0.2-0.3 mL/kg • Fluid produced by systemic vessels of the parietal pleura, primarily less dependent capillaries, based on: • Permeability of the pleural vessels • Hydrostatic and oncotic gradients • Fluid removed by pleural lymphatics in dependent portions of parietal pleura • Rate of production at homeostasis: 0.1 mL/kg/h Theodore et al, 2010; Suratt, 2003; Noppen et al, 2000
Normal Pleural Fluid Composition • Low in protein: <100 mg/dL • Slightly alkaline compared to serum: pH = 7.60-7.64 • Hypocellular compared to serum • 1000-2000 WBC/μL • 75% macrophages (IR 64-81%)* • 23% lymphocytes (IR 16-31%)* * Median values; IR= interquartile range Suratt, 2003; Noppen et al., 2000
Mechanisms of Pleural Effusion • Increased pulmonary capillary pressure (CHF) • Increased pulmonary capillary permeability (PNA) • Decreased intrapleural pressure (Atelectasis) • Decreased plasma oncotic pressure (Hypoalbuminemia) • Increased pleural membrane permeability and obstructed lymphatic flow (pleural malignancy, infection) • Diaphragmatic defects (hepatic hydrothorax) • Thoracic Duct Rupture (chylothorax) Porcel and Light, 2006
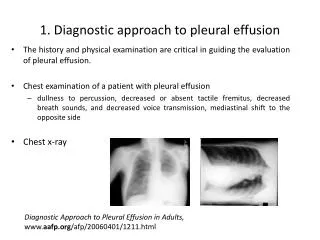
Symptoms and Exam Findings Symptoms • Dyspnea • Often disproportionate to hypoxemia • Cough • Pleuritic Chest Pain Physical Exam • Decreased breath sounds • Dullness to percussion • Decreased tactile fremitus • Egophony (EA) • May find rales or pleuritic friction rub
Chest Radiography • >50-75 mL of fluid on lateral radiograph to blunt costophrenic angle • >175-200 mL of fluid on P/A view to blunt lateral costophrenic angle • Clinically significant pleural effusion: >10mm fluid present on lateral decubitus radiograph (or U/S)
Diagnostic Workup • Delayed thoracentesis in parapneumonic effusion associated with: • Longer hospital stay • Greater healthcare cost • Initial pleural fluid analysis: • Protein • LDH • Cell count with differential • Gram stain/culture • Glucose • Cytology • pH Heffner et al, 1995; Light, 2002
Transudate versus Exudate? Light, 2002
Transudate versus Exudate? DDx Suratt, 2003; Ansari and Idell, 1998; Light, 2006
Role for CT scan in Workup? • CT has higher sensitivity than CXR or MRI for: • Pleural thickening and loculation • Pleural vs. parenchymal disease • Empyema vs. abscess • Pulmonary embolism • Helical CT • Malignancy • Mediastinal disease Porcell and Light, 2006; Davies et al, 2003; Qureshi and Gleeson, 2006; Sahn, 2007
Role for CT scan in Workup? • However, there are no trials demonstrating benefits of CT in terms of: • Shorter time to diagnosis • Decreased need for diagnostic procedures (e.g. thoracentesis) • Shorter hospital stay/decreased cost • Management guidelines recommend CT scans for complicated cases after failed initial diagnostic workup Porcell and Light, 2006; Davies et al, 2003; Qureshi and Gleeson, 2006; Sahn, 2007
Other Diagnostic Testing • Ultrasound • Guided thoracentesis • Identifies locultated effusion • Needle biopsy of pleura • Tuberculouspleuritis and malignancy • Bronchoscopy • Bronchial invasion by malignancy or infiltrate • Thoracoscopy • Allows for pathologic analysis • Option for pleurodesis • Open biopsy Davies et al, 2003; Light, 2006; Sahn, 2007
Summary • Pleural fluid is produced and removed by parietal pleura • Multiple mechanisms to disrupt homeostasis • Thoracentesis essential to diagnosis • Light’s criteria: sensitive and specific for identifying exudative effusions • CT scan can be helpful for complicated cases
References • Theodore PR, Jablons D. Chapter 18. Thoracic Wall, Pleura, Mediastinum, & Lung. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 13e.New York, NY: McGraw-Hill; 2010. http://accessmedicine.mhmedical.com.liboff.ohsu.edu/content.aspx?bookid=343&Sectionid=39702805. Accessed April 18, 2014. • Suratt BT. Chapter 22. Pleural Effusions, Excluding Hemothorax. In:Hanley ME, Welsh CH. eds. CURRENT Diagnosis & Treatment in Pulmonary Medicine. New York, NY: McGraw-Hill; 2003. http://accessmedicine.mhmedical.com.liboff.ohsu.edu/content.aspx?bookid=346&Sectionid=39883273. Accessed April 18, 2014. • Noppen M, De Waele M, Li R, Gucht KV, D’Haese J, Gerlo E. Volume and Cellular Content of Normal Pleural Fluid in Humans Examined by Pleural Lavage. Am J RespirCrit Care Med 2000; 162: 1023-1026. • Porcel JM, Light RW. Diagnostic Approach to Pleural Effusion in Adults. Am Fam Physician 2006; 73: 1211-1220. • Heffner JE, McDonald J, Barbieri C, Klein J. Management of Parapneumonic Effusion: an analysis of physician practice patterns. Arch Surg1995; 130:433-438. • Light RW. Pleural Effusion. NEJM 2002; 346: 1971-1977 • Ansari T, Idell S. Management of Undiagnosed Persistent Pleural Effusion. Clin Chest Med 1998; 19(2): 407-417. • Light RW. The Undiagnosed Pleural Effusion. Clin Chest Med 2006; 27: 309-319. • Qureshi NR, Gleeson FV. Imaging of Pleural Disease. Clin Chest Med 2006; 27: 193-213. • Davies CWH, Gleeson FV, Davies RJO. BTS Guidelines for the management of pleural infection. Thorax 2003; 58(ii): 18-28. • Sahn SA. Diagnosis and Management of Parapneumonic Effusions and Empyema. Clin Infect Disease 2007; 45: 1480-1486. • Light RW. Pleural Effusions. Med Clin N Am 2011; 95: 1055-1070