Download
1 / 36
380 likes | 980 Views
PARKINSON’S DISEASE. Donald R. Noll DO FACOI e dited by Dr. Edward Warren Chair, Geriatrics Carolinas Campus May 2012. Describe the clinical manifestations of Idiopathic Parkinson’s Disease List the medications for Parkinson’s Disease and their common side effects.

E N D
PARKINSON’S DISEASE Donald R. Noll DO FACOI edited by Dr. Edward Warren Chair, Geriatrics Carolinas Campus May 2012
Describe the clinical manifestations of Idiopathic Parkinson’s Disease List the medications for Parkinson’s Disease and their common side effects. Discuss the clinical evidence for using OMT in Parkinson’s Disease Describe the clinical features and characteristics of other causes of Parkinsonism. Objectives
Parkinson’s is a common condition, with multiple causes and varieties. The most common variety is Idiopathic Parkinson’s Disease (paralysis agitans). This one affects all ethnic groups and has an approximately equal gender distribution. It usually begins at age 45 to 65. The cardinal manifestations of Parkinsonism are Tremor, Rigidity, Bradykinesia, and Postural Instability. General Considerations
It is caused by degeneration of the dopaninergicnigrostriatal system. There is a dopamine deficiency. This leads to a disturbance in motor function. Treatment is directed at restoring balance, by blocking acetylcholine or increasing dopamine. Toxins, head trauma (boxing), and other causes of neuronal damage in the substantia nigra have been blamed for it. Etiology
Cell Loss in the SubstantiaNigra The midbrain on the left from a Parkinson’s patient shows a pale substantianigra (red arrows). A normally pigmented midbrain is seen on the right (yellow arrows).
Decline in cognitive function. This varies in other forms of Parkinsonism. Serious cognitive decline is a late manifestation of Idiopathic Parkinson’s Disease, while it is an early manifestation of Lewy Body Dementia (and other degenerative dementias). Tremor is at about 4 to 6 cycles per second, it is worse at rest, it is enhanced by emotional stress, and is often less severe with voluntary activity. Classically, the tremor may be unilateral for months or even years, but can present bilaterally. Some patients present with no tremor. More clinical features
“Pill Rolling” Tremor Historical Point: There are no more “pills”. The last one ended in the 1970’s. They were medicines dispersed uniformly through dough which was then cut uniformly to make predictable doses. These pieces of dough were then rolled into balls using the thumb, index, and middle fingers. This is the etymology behind the “pill rolling” tremor.
The cardinal symptom of Parkinson’s. Initiation of movement is delayed or slowed. It causes the flexed, bent over posture, decreased mobility. Voluntary and automatic movements are reduced, such as the normal arm swing during walking. Normal voluntary movement may be suddenly, but briefly restored during an emergency (example: leaping out of the way of a speeding car) Bradykinesia
Cogwheel Rigidity Cogwheel quality, because when an extremity is moved passively, there is resistance that stops and starts in a quick repetitive sequence.
Parkinson’s Gait • Marked by shuffling, short steps • Stooped posture • Reduced arm swing • Arm and hand tremor may be accentuated while walking • Slow initiation (bradykinesia) • Festinating gait (difficulty stopping)
Postural Instability • Late manifestation of Parkinsonism • Highly disabling • Falling forward (“propulsion”) • Falling backward (“retropulsion”) • Spontaneous loss of balance
Masklike Facies Masklike facies: Loss of facial expression can create the appearance of apathy and depression: a stolid, unmoving expression.
Constipation is frequent and often worsened by therapy Orthostatic hypotension Sexual dysfunction Urinary incontinence Excessive sweating Sleep disturbances, including daytime drowsiness, insomnia, REM sleep disturbance Restless legs syndrome are present in 74%–98% of patients Unsteadiness on turning Poorly modulated voice Mouth drooling (advanced stage) Swallow dysfunction (a life threatening problem late in the disease) Parkinson’s Dementia (late in the disease, 80% get it) Other Symptoms
No therapy has been shown to slow disease progression. In the early stages, no drug therapy is required, because, the effectiveness of most lessens over time (last only 10 years). Waiting to use drug therapy until symptoms become significant is a valid management strategy. Most drugs for Parkinson’s Disease have significant side effects, so treatment needs to be monitored carefully. Many people who are on Parkinson’s medication do not have the disease. Be skeptical about it. Treatment: General Comments
For patients with mild symptoms It improves all symptoms of Parkinsonism Its mode of action is unclear Side effects: Rare, but can be serious. Dose: Use 100mg bid. Restlessness Confusion Anorexia Postural hypotension Cardiac arrhythmias Amantidine
These drugs are poor choices. They may help the tremor and rigidity, but are generally not effective. Examples: benztropine, trihexyphenidyl, orphenadrine Side Effects: These are both common and severe in the elderly. Dry mouth, nausea, constipation, cardiac arrhythmias, palpitation, urinary retention, confusion, agitation, and increased intraocular pressure. If you decide to use an anti-cholinergic drug, then start at the lowest dose, observe and slowly work the dose up to an effective dose. If no significant clinical response, then discontinue the medication. Anti-cholinergic Drugs
Levodopa – helps all major features of Parkinsonism: converted to dopamine in the body. Carbidopa – inhibits the enzyme which breaks levodopa down, and since it does not cross the blood brain barrier, it lowers the amount of levodopa required to get a therapeutic effect. This makes the treatment more tolerable, since most side effects of Levodopa are dose related. Remember: high protein meals interfere with the absorption of Levodopa, causing fluctuations in symptoms. Start with Sinemet 25/100 (carbidopa 25 mg/ levodopa 100 mg) tid and adjust clinically. Using Sinemet CR (controlled release) may help with compliance and symptom fluctuations. Levodopa/Carbidopa
Levodopa/Carbidopa Side Effects Most commonly - Nausea, vomiting, and hypotension Psychosis: Levodopa is relatively contraindicated in psychosis and in dementia related neurobehavioral disturbances. Psychosis in a Parkinson’s patient should first be treated by stopping the Parkinson’s medications. Cardiac arrhythmia Restlessness Confusion Dyskinesia shows up as frank chorea, athetosis, tremor, tics, or myoclonus On-Off phenomenon – later in the disease: unpredictable sudden changes drug effectiveness
Act on dopamine receptors in the brain. They can be used early or late in the disease, with or without levodopa/carbidopa therapy. Bromocriptine – an ergot – can cause nausea, vomiting, constipation and postural hypotension. Pramipexole and ropinirole- cause fatigue, somnolence, nausea, peripheral edema, dyskinesias, confusion, and postural hypotension. Dopamine Agonists
Adjunctive therapy, good for helping fluctuations. Or use early in the disease. Rasagiline – 1 mg daily Selegiline - 5 mg daily in am and at noon Avoid tyramine - rich foods (wine & cheese), can cause a hypertensive crisis. Selective Monoamine Oxidase Inhibitors
Selegiline is a selective inhibitor of monoamine oxidase type B which metabolizes dopamine. There was considerable interest in the use of selegiline as a neuroprotective agent given the results of the DATATOP study (NEJM 1989;321:1364-1371). However, there has been considerable controversy over the interpretation of these results. It does not appear to be true. Secondly, there has been some suggestion that the use of selegiline is associated with increased mortality (BMJ 1995;311:1602-1607). This has been shown in one study, however, the causes of death are unknown at present. More on Selegiline
Catecholamine-O-methyltransferase inhibitors These reduce the metabolism of levodopa to 3-O-methyldopa, thus improve the pharmacokinetics of levodopa. Tolcapone and entacapone – use as adjunctive therapy to levodopa/carbidopa. When starting, reduce the dose of levodopa-carbidopa by about 1/3 to avoid dyskinesia, confusion, hypotension and syncope. Diarrhea is a common side effect. Rarely – patients have liver failure with tolcapone (avoid in liver disease and monitor liver enzymes) No liver problem yet reported with entacapone. Stalevo® is a commercial preparation of carbidopa and levodopa and entacapone. COMT Inhibitors
For Parkinson’s Disease • Wells MR, Giantinoto S, D’Agate D, Areman, Fazzini E, Dowling D and Bosak A • Standard osteopathic manipulative treatment acutely improves gait performance in patients with Parkinson’s Disease • JAOA Vol. 99 (No. 2) February 1999 • Winner of the JAOA best paper award for the year 2000. • A PDF copy of this paper can be downloaded at http://www.jaoa.org/ then search for the article by author, key words or date.
Details of the study • Three groups or experimental arms • Treatment, sham & normal • All subjects had a 12 hour medication washout prior to treatment • The OMT protocol used multiple techniques • 14 OMT techniques • The sham was Range of Motion • To measure effect, computer aided gait analysis was used • The magnitude of change was compared
Results: • Age 45 - 68, 10 OMT subjects, 10 sham, 8 age matched controls • Treated group – significant improvement in stride length and velocity of upper and lower extremities – between group analysis • No change in normal and sham groups
OMT and Parkinson’s DiseaseBefore and after pictures Before OMT After OMT
Always, always, every visit look at the medications and ask yourself is the problem can be blamed on the drugs. Metaclopramide (Reglan®) is commonly used for treating GERD or diabetic gastroparesis. It improves gastric motility and emptying by inhibiting dopamine. Anti-psychotic medications all can cause Parkinsonism – mostly a dose related side effect. Drug Induced Parkinsonism
The third most common cause of degenerative dementia. Produces a clinical picture of dementia with Parkinsonism. The dementia comes earlier than in Parkinson’s disease. Cognition waxes and wanes more. These patients are very sensitive to anti-psychotic medications. Both Idiopathic Parkinson’s Disease and Lewy Body Dementia patients have Lewy Bodies. There are more in the dementia. Key point: Medications for Idiopathic Parkinson’s Disease work poorly in Lewy Body Dementia. Parkinson’s medications often cause falls and psychosis in these patients. Use them with caution and discontinue them if no significant improvement found after a therapeutic trial. Lewy Body Dementia
All the manifestations of Parkinson’s Diseases plus systemic autonomic failure: postural hypotension dizziness cerebellar dysfunction gastroparesis cardiac arrhythmias frequent falls They respond to medications for Parkinson’s, but they tolerate the side effects poorly. Shy-Drager Syndrome
Normal aging – some (very mild) bradykinesia and tremor occur with aging – NOT Parkinson’s Depression – can cause psychomotor retardation and a masklike facies, which could be confused for Parkinsonism Huntington’s Disease – has a strong family history, unlike Parkinson’s Disease Creutzfeldt-Jakob disease – a progressive dementia, EEG fairly specific Postencephalitic Parkinson’s - rare these day Toxin Exposure – manganese, carbon disulfide or carbon monoxide poisoning MPTP induced – see next slide Related Conditions
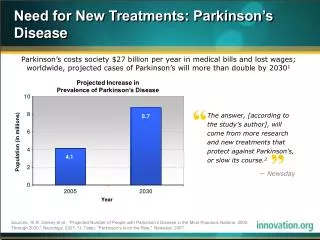
The recognition that exposure to the neurotoxin 1-methyl, 4-phenyl, 1,2,3,6-tetrahydropyridine (MPTP) can cause a syndrome clinically and pathologically similar to Parkinson’s continues to foster interest in other environmental risk factors. A number of such factors, including heavy metals, well water, pesticides, and rural versus urban residence have been evaluated. In most cases, the increased risk from these exposures were modest. Environmental Risk Factors for PD
Resources • 2008 Current Medical Diagnosis and Treatment, SJ McPhee and MA Papadakis, page 867 to 870. • John Paulus D.O. 2006-2007 Core Geriatrics Rotation Lecture on Parkinson’s Disease