Download
1 / 39
560 likes | 1.96k Views
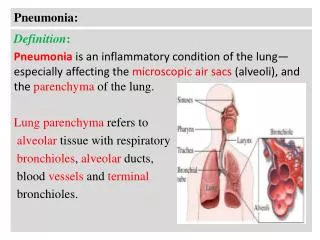
Pediatric Pneumonia. Pisespong Patamasucon,M.D Pediatric Infectious Diseases. Leading Etiologic Agents of Pneumonia Infants and Children. Clues to The Etiology of Pneumonia Obtained Through History – Taking. Clues to The Etiology of Pneumonia Obtained Through History – Taking ( con’t).

E N D
Pediatric Pneumonia Pisespong Patamasucon,M.D Pediatric Infectious Diseases
Clues to The Etiology of Pneumonia Obtained Through History – Taking
Clues to The Etiology of Pneumonia Obtained Through History – Taking ( con’t)
Diagnostic Tools for pneumonia • CXR • Sputum culture • Blood culture • Urine antigen test – CIE or latex agglutination • Lung tap • Pleural fluid culture
Epidemiology,Clinical,and Laboratory Features of Acute Pneumonia in Normal Infants and Children According to Etiologic Agents
Epidemiology,Clinical,and Laboratory Features of Acute Pneumonia in Normal Infants and Children According to Etiologic Agents (con’t)
Epidemiology,Clinical,and Laboratory features of Acute Pneumonia in Normal Infants and Children According to Etiologic Agents (con’t)
Epidemiology,Clinical,and Laboratory Features of Acute Pneumonia in Normal Infants and Children According to Etiologic Agents (con’t)
Etiology of Pneumonia in infants and Children Winter Viral Agents Para 1,2,3 Influenza A,B Etc. S.Pneumonia Mycoplasma Summer RSV C.Trachomatis CMV 1° Staph. Strep.Gr.B E.coli 2°Staph. C. pneumoniae H.Inf.B. 3 yrs. 5 yrs. 10 yrs. 6 mo. 1 mo. 3 mo. 1 yr.
Prospective Studies of Perinatal Chlamydia Infection Infants City Mother Conjunctivitis(%) Pneumonia (%) San Francisco 5 18 16 Seattle 13 44 -- Denver 9 44 22 Boston 2 33 17 Seattle 12 33 8 Lund 9 22 -- Nairobi 22 37 12
Clinical Features of C. Trachomatis Pneumonia • Onset at 3 to 11 wks of age • Cough greater than one week in duration • Prior conjunctivitis • Afebrile tachypnea with diffuse rales • Hyperinflation and interstitial infiltrates on chest film • Eosinophilia • Increased IgM • Increased IgA and IgG
Number of patients Treatment day Treatment day when improvement first noted
Pneumococcal pneumonia Most common in late winter or early spring during the peak of viral infection • Abrupt onset of fever • Restlessness • Respiratory distress following URI
Physical exam & Labs Diminished B. S or fine, crackling rales Neck rigidity without meningitis may occur (RUL) WBC 15,000 - 40,000 Blood C/S positive only 30% Lobar consolidation (less common in infants) Para-pneumonic effusion is relatively common
Mycoplasma pneumoniae in the United States Syndrome Incidence/year Total cases Pneumonia 2/1.000 500,000 Tracheobronchitis 46/1,000 11,500,000 Asymptomatic 12/1,000 3,000,000 Infections All infections 15,000,000
Incubation Clinical illness Convalescence 0 3 4 5 6 Wks.-2 -1 1 2 Symptoms: Headache,malaise Fever Sore throat Cough Signs: Sputum Dullness Rales Laboratory: Positive culture x-ray
Chlamydia pneumoniae ( TWAR ) This organism cause pneumonia, bronchitis,sinusitis and pharyngitis and is a common cause of infection in children from the age 5 – 15 years. Of the three Chlamydia species, Chlamydia pneumonia is by far the most common cause of human infection
Clinical Finding inPneumonia Associated with M.Pneumoniae,TWAR and Viral Respiratory Agents
Outpatient 0-20 days Admit pt. 3wks-3mos Afebrile; give PO erythromycin. Admit for fever or hypoxia 4mos-4yrs PO amox or azithro. If >8 yrs, PO doxycycline (4mg/kg/day, 2 divided doses) Inpatient (septic, alveolar infiltrate, large pleural effusion or all) 0-20 days IV amp/gent with or w/o IV cefotaxime 3wks-3mos Give IV cefotaxime or ceftriaxone 4mos-4yrs IV cefotaxime, ceftriaxone, if pt not well consider IV azithromycin*
Pleural Empyema In Children Stages of infection Exudative (allows needle aspiration) Fibrinopurulent (may be loculated) Organizing Treatment options Exudative Repeated needle aspiration (1-5 days) Exudative or Chest tube drainage fibrinopurulent Organizing Decortication If >50% limitation of lung shown by CT scan After 2-4 weeks of medical management tachypnea, asymmetry of chest wall expansion, fever,or leukocytosis remain
Algorithm for Empyema Thoracentesis Gram stain-neg Gram stain-pos Pleural effusion Observe Chest tube Resolution Increasing fluid Resolution Non-resolution Open drainage Decortication
Which of the following statements regarding pneumonia in children is true? • A .Specific microbial pathogen usually can be identified • B. All children who have pneumonia should be hospitalized for observation and treatment • C. Pneumonia is a rare cause of child mortality worldwide • D. Radiographs of the chest always should be obtained to determine the cause • E. Viral agents are the most common causes of pneumonia in older infants and children
You are evaluating an 8 year old boy who has 7 day history of malaise and worsening cough. His mother reports that he has had low grade fever. PE reveals a well appearing boy with normal RR and pulse ox. Lung exam reveals bilateral crackles without wheezing . Chest x-ray show bilateral interstitial infiltrates without effusion. • Most likely pathogen is: • A. Haemophilusinfluenzae • B. Mycobacterium tuberculosis • C. Mycoplasmapneumoniae • D. Respiratory syncytial virus • E. Streptococcus pneumonia
An 8 week old girl presents to ER with increased work of breathing x 1 day. Temp of 101.1 F, difficulty breastfeeding due to nasal congestion. RR 70, pulse ox 90% on RA. Lung exam reveals bilateral wheezes and crackles. CXR shows increased perihilar markings bilaterally and right middle lobe opacity. • Most likely cause of her symptoms is; • A. Adenovirus • B. Bordetella pertussis • C. Chlamydia trachomatis • D. Group B Streptococcus • E. Respiratory syncytial virus
#4 Main Cause of Necrotizing Pneumonia is: • Streptococcal hyaluronidase • Teichoic acid • Pneumolysin • Fibrinolysin • Ponton-valentine leukocidine
#5 The following microorganisms are frequent causes of pleural effusion EXCEPT: • S. aureus • Strep pneumoniae • Group A streptococcus • Haemophilis influenzae type B • Mycoplasma pneumoniae
#6 Characteristics chlamydial pneumonia include the following EXCEPT: • Afebrile • History of conjunctivitis • Staccato cough • Eosinophilia • Present at 4-6 months of age
#7 Distinguish features of exudate from transudate are as follows EXCEPT: • Pleural fluid: serum protein ratio > 0.5 • Pleural fluid LDH > 200 IU/ml • Pleural fluid: serum LDH > 0.6 • Pleural fluid protein > 3 gm/ml • Leukocyte count > 1,000/CU/mm
Features Differentiating Exudative & Transudative Pleural Effusion TransudateExudate • WBC <10,000/mm³ >50,000/ mm³ • pH >7.2 <7.2 • Protein <3.0 g/dL >3.0 g/dL • Protein ratio <0.5 >0.5 • LDH <200 IU/L >200 IU/L • LDH ratio <0.6 >0.6 • Glucose ≥60 mg/dL <60 mg/dL