Download
1 / 17
171 likes | 319 Views
(A rare case of) Segmental A r terial Mediolysis. Shenouda M, Riga C, Naji Y, Renton S. KSS Core Surgery Prize Day Friday 4th January 2013. Mrs X, 85 y/o. PC – acute onset epigastric pain Sharp, associated with nausea, vomiting, sweating. N o haematemesis/melaena; no neck/chest pain

E N D
(A rare case of) Segmental ArterialMediolysis Shenouda M, Riga C, Naji Y, Renton S KSS Core Surgery Prize Day Friday 4th January 2013
Mrs X, 85 y/o • PC– acute onset epigastric pain • Sharp, associated with nausea, vomiting, sweating. • No haematemesis/melaena; no neck/chest pain • No previous episodes • PMHx– 2 previous visceral aneurysm repairs (15y previously), HTN, recent NSTEMI • FHx– IHD • SHx– lives alone, independent, active, ex-smoker (50-pack years – stopped 6/12 previously)
O/E • Alert, orientated, GCS 15/15 • Stable vital signs: Temp 35.8, HR 52, BP 132/53, RR 18, SaO2 96% O/A • Pale, clammy, otherwise normal CVS/resp ex • Abdo: midline scar; severe epigastric/central tenderness with guarding. No pulsatile masses, absent bowel sounds • Peripheral vasc: No signs of acute ischaemia All pulses present No radio-radial or radio-femoral delay CRT <2 sec in all four limbs • Neurology intact
Basic Ix • Urine NAD, ECG - SR • Bloods– Hb 9.2, WCC 16.2, Plt 183, Clot NAD, CRP <5 • Cr 81, Ur 7.4, Na 141, K 4.7, Trop 0.13 • Clotting, LFTs NAD Urgent CT Angio….
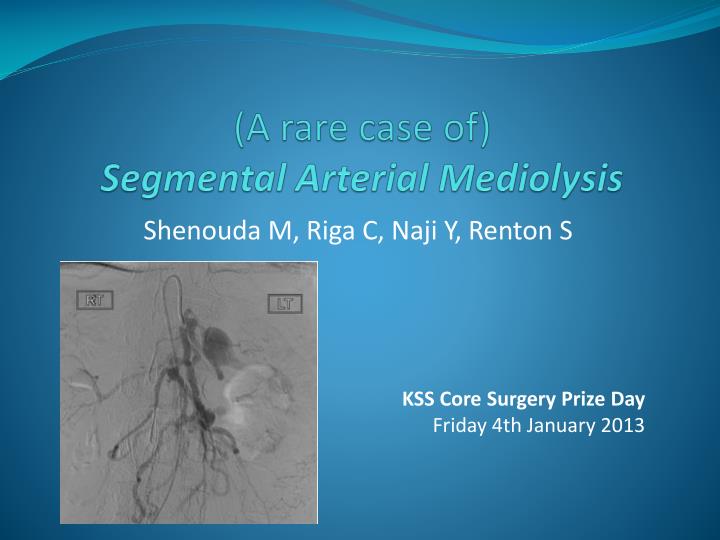
CTA • 11 mm aneurysm arising from a branch of the gastroduodenal artery is seen with surrounding haematoma, suspicious for rupture. • Difficult anatomy is seen with common trunk for the celiac and SMA, and a 10mm aneurysm in SMA trunk. • Multiple other aneurysms –25mm splenic artery aneurysm, 14mm aneurysm at the origin of the IMA.
Management • Cross-matched 6 units, fluid resuscitation • Urgent angiogram…
Angiogram & Embolisation • LA, R CFA puncture • Selective catheterisation of the celiac axis and then GDA cannulated. The aneurysm was identified. Embolisation with several microcoils proximal and distal to the aneurysm in the GDA; complete cessation of flow within the aneurysm. • Findings in keeping with CTA –multiple visceral aneurysms. • Also noted multiple narrowings and irregularities in the visceral arteries.
SEGMENTAL ARTERIAL MEDIOLYSIS • 1976 – • Slavin RE, Gonzalez-Vitale JC. Segmental mediolytic arteritis. A clinical pathologic study. Lab Interv 1976;35:23–91. • Described 3 autopsy cases • partial or total mediolysis arterial gaps dissecting aneurysms rupture massive haemorrhage • 85 cases in literature • Abdominal visceral arteries, intracranial arteries • Aetiology unknown
SEGMENTAL ARTERIAL MEDIOLYSIS • Presentation – • intra-abdominal/intracranial haemorrhage • asymptomatic on routine investigations • post-mortem • Diagnosis – • radiological – arterial dilatation, single/multiple aneurysms, stenoses/occlusion, dissection • histological – surgical resection, post-mortem
SEGMENTAL ARTERIAL MEDIOLYSIS • Literature review, 1976-2012 • 62 studies, 85 cases • 69% confirmed histologically (24% on autopsy) • M:F – 1.5:1 • Age range 0-91 (median 57) • 21% had history of hypertension • 13% mortality before further investigation/management • Overall mortality 25% • Management – open vs endovascular
Summary • SAM is a rare diagnosis of unknown aetiology • May be asymptomatic or present with massive haemorrhage • Treatment usually restricted to symptomatic cases • Endovascular embolisation can prevent the need for major surgery • Can also be a temporary measure before definite surgery at a later stage
References • Slavin, RE. Gonzalez-Vitale, JC. Segmental mediolytic arteritis: a clinical pathologic study. Lab Invest 1976; 35:23–29. • Michael, M. Widmer, U. Wildermuth, et al. Segmental arterial mediolysis: CTA findings at presentation and follow-up. AJR Am J Roentgenol 2006; 187:1463-9 • Tameo, MN. Dougherty, MJ. Calligaro, KD. Spontaneous dissection with rupture of the superior mesenteric artery from segmental arterial mediolysis. J Vasc Surg 2011;53:1107-12.