Download
1 / 33
330 likes | 470 Views
Laboratory Evaluation of Renal Function. S .POPLI. M.D.,F.A.C.P. 7/13/2005. Proteinuria Case 1. A 20 year old patient is referred to you for ,he has been diabetic for 6 years ,he was told to have some kidney problem by his MD.He wants to know the cause of renal dysfunction.

E N D
Laboratory Evaluation of Renal Function S .POPLI. M.D.,F.A.C.P. 7/13/2005
Proteinuria Case 1 • A 20 year old patient is referred to you for ,he has been diabetic for 6 years ,he was told to have some kidney problem by his MD.He wants to know the cause of renal dysfunction. • GPE:BP 145/90 ,otherwise exam is normal • How would you proceed ? • BUN 15mg/dl, creatinine 1.0mg/dl ,U/A shows SG 1.024 ,trace protein ,a few hyaline casts • What test would you order next ? • 24h protein collection , U protein/U creatinine ratio or both?
Case 1 continued • Urine protein /Urine creatinine returns 15mg/150mg ratio(<0.1) • Does this patient have abnormal proteinuria ? • Patient wants to know if he has microalbuminuria ,you order urine micro albumin result is :60mg micro albumin /gm creatinine . • Is this abnormal, does this patient have diabetic nephropathy?
Urine Protein:Categories of persistent proteinuria • Overflow: Capacity to reabsorb normally filtered protein in proximal tubules over whelmed due to overproduction:e.g.light chains,hemoglobinuria and myoglobinuria • Tubular proteinuria: Decreased reabsorption of filtered proteins by tubules due to tubulointerstitial damage ; usually <2 gm • Glomerular proteinuria: Microalbuminuria to overt proteinuria usually>3.5 gm
Screening for Urine protein • Dipstick: Gives green color, does not check for light chains Negative – 10 mg/dl Trace – 15-25 mg/dl 1-2+ – 30-100 mg/dl 3+ – 300 mg/dl • Sulfosalicylic acid: white precipitate
Urine protein :Quantitative measurement • 24 hour collection of urine for protein normal excretion is <150 mg/24 hour • Spot urine protein/urine creatinine ratio : (as 24 h urine creatinine excretion is a function of muscle mass i.e. 15 mg/kg for females and 20mg/kg for males ) a normal ratio is 150/1500 or <0.1 . A ratio >3 indicates nephrotic range proteinuria • Case 1 has normal urine protein excretion, trace protein on u/a is due to highly concentrated urine ,pt may still have microalbuminuria
Microalbuminuria • Urine albumin excretion below detection by regular dipstick • First clinical sign of diabetic nephropathy • Incidence increases with the duration of diabetes and may be present at the diagnosis of NIDDM • Transient albuminuria may occur with fever,infection,exercise,decompensated CHF • Associated with poor glycemic control and elevated BP
Detection of Micro albuminuria: 24 hour urine collection • Normal urine protein excretion : <150mg (20% of this is albumin) • Therefore, normal urinary albumin excretion is < 30 mg/day • Microalbuminuria :urinary albumin excretion 30-300 mg/day
Microalbuminuria :Detection by Spot Urine Albumin to Urine Creatinine ratio • Easier than cumbersome 24 hr.collection • If we assume daily creatinine excretion to be 1000 mg and normal urine albumin excretion <30 mg; albumin / creatinine ratio should be less than 0.03 or 30mg/g creatinine • Thus case 1 has micro albuminuria which is likely due to diabetic nephropathy.How would you manage him now?
Why and When to Screen Patients for Microalbuminuria ? • BP control with Ace_I and ARB’s have been known to reduce microalbuminuria and delay the progression of kidney disease in diabetics • IDDM patients should be screened yearly,beginning 5 years after the onset of disease • Patients with NIDDM should be screened at presentation
Proteinuria Case 2 A70 year- old male is referred for chronic azotemia PMH: unremarkable GPE: BP120/60 , LE edema Labs: U/A SG 1.010 pH 6.0 , protein neg, glucose 2+, Uprotein /U creatinine ratio 4 BUN 30mg/dl creat.3.0, Blood Sugar 78mg/dl albumin 2.8, Hb 10 gm What other tests would you order to diagnose cause of his renal dysfunction ? UPEP,why?
Clinical Assessment of Renal Function: Glomerular Filtration Rate(GFR) • Parameters used Blood urea nitrogen Serum creatinine Endogenous creatinine clearance
Case 3 Azotemia • A 55 year old diabetic female is admitted with intractable vomiting and low urine output • Exam: BP 120/60 with postural hypotension • Labs: BUN 60, Creat. 2.0 mg/dl ( baseline 1.0mg/dl), Hb 16gm • ,U/A: SG 1.020, sediment: hyaline casts,UNa: 10 mmol/L,UOsm: 600 mosm/kg,Ucreat.150mg/dl ,Fe Na < 0.5 • Q.What is the cause of her high BUN to creatinine ratio and her renal failure? What are the other causes of high BUN to creatinine ratio
Blood Urea Nitrogen (BUN) • Catabolism of aminoacids generates NH3 NH2 2 NH3 + CO2 = C = 0 + H2O NH2 • Urea Mol wt : 60 • BUN Mol wt. : 28 • Normal BUN 10-20 mg/dl • After filtration › 50% is reabsorbed by the tubule • BUN level is related to: Renal function, protein intake, and liver function
Creatinine • Formed at a constant rate by dehydration of muscle creatine • Normally 1–2% of muscle creatine is broken into creatinine • Mol. Wt. 113 • Creatinine is freely filtered by the glomerulii and is not reabsorbed 10–15% is secreted into proximal tubule
Creatinine • Normal serum level 1–2 mg/dl • 24 hour creatinine excretion 20 mg/kg/day for males 15 mg/kg/day for females • Children, females, elderly, spinal cord injured have low serum and urine creatinine
BUN/Creatinine ratio 10:1 • Normal • Chronic renal failure
D/D in Case 3 with BUN Creatinine ratio >10:1 • Decreased perfusion • Hypovolemia • Congestive heart failure • Increased urea load • GI bleed • Glucocorticoids -Tetracycline • Hyper catabolic states • High Protein diet • Obstructive uropathy • Decreased muscle mass
Pathophysiology of Pre-renal Azotemia in Case 3 Decreased “Effective” Intravascular ADH Volume + Renal Hypoperfusion activation of RAS Diminished GFR aldosterone Low urine volume and U sodium and high Uosmolality
Case 3 :Diabetic patient continued.. • Vomiting stopped ,BP improved and BUN/creat lowered to 35/1.8mg/dl. 24 hours later she developed UTI, trimethaprim/sulfamethoxazole was started • Next day 24 hr urine output 800 mL • Exam: Unremarkable • BUN: 20 mg/dl Creat: 3.0 mg/dl • Uosm: 600 mosm/kg ,UNa: 10 mom/l, FeNa: <1% • Urine Sediment: Hyaline casts • What is the cause of < 10: 1 ,BUN to creat ratio now?
BUN/Creatinine ratio ‹ 10:1 • Decreased urea load Low protein diet Liver failure • Inhibition of creatinine secretion Cimetidine Trimethoprim Probenecid • Increased removal: Dialysis
BUN/Creatinine ratio ‹ 10:1 • Increased creatinine load Ingestion of cooked meat Rhabdomyolysis • Interference with creatinine measurement Ketosis Cefoxitin • Increased muscle mass Anabolic steroids Muscular development
Case 3 continued… 6 months later • Pt was discharged with normal BUN and creatinine,6 months later she is admitted with vague abdominal pain, an US done shows 6 cm abdominal aortic aneurysm, she undergoes resection with cross-clamping of aorta for 2 hours. • Post surgery she is oliguric (u/o less than 70ml in 8 hours).On exam well hydrated. • U/A: SG 1.015 ,”Dirty brown sediment “U Na 40 mEq /L U osmolality 350 mOsm/l ,Fe Na 2% • What is your diagnosis after reviewing the lab data ? How would you manage?
Urinary Indices in Diagnosis of Acute Renal Failure Pre renal ATN Uosm(mosm/kgH20) >500 <350 Urine sodium (mmol/l) <20 >40 Urine/plasma urea nitrogen >8 <3 Urine/Plasma Creatinine >40 <20 Fractional Excretion of Sodium<1% >1% Sediment normal “dirty brown”
Fractional Excretion of filtered Sodium(FeNa) • FeNa= Amount of Na excreted Amount of Na filtered • FeNa=UNa x Urine volume PNa x GFR • FeNa = UNa x V PNa x[(UCr x V) /PCr] • FeNa % =UNa x PCr X 100 PNa x UCr
Case 4 • 20 y/o male is seen at West point ,on admission physical : wt 70Kg , BUN 10mg/dl, serum creatinine 1.0mg/dl, GFR was 100ml/min and he excreted 1500mg creatinine /day in the urine. 2 months later he develops acute glomerulonephritis with RBC and fatty casts.His serum creatinine increases to 2mg/dl and remains at 2mg/dl at 1 year follow up .Wt is 72kg • What is his estimated GFR by Cockcroft and Gault formula and by serum creatinine? • What would be the creatinine excretion now at 1 year ?
Concept of Clearance ? Measurement of GFR by Creatinine Clearance(Ccr) • Urine is collected for 24 hours and plasma creatinine is measured the next day • 1. Filtered creatinine = Excreted creatinine • 2. GFR x Pcr = Ucr x Volume • 3. GFR = Ucr. mg/dl x V ml Pcr.mg/dl • Normal GFR = 100 ml/min • GFR declines by 1 ml/min/year after age 40
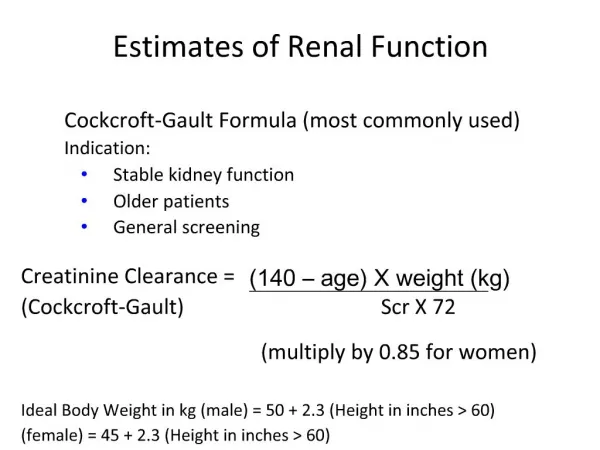
GFR Estimation by Plasma Creatinine • Cockcroft and Gault Formula* Calculated creatinine clearance = (140–age) x wt (kg) 72 X serum creatinine(mg/dl) For females, subtract 15% (or multiply by 0.85); for paraplegics multiply by 0.8, for quadriplegics, multiply by 0.6 Est GFR for this pt is .. (140-20)x70 72x2 *Applicable only when patient is in a steady state, not edematous and not obese
GFR Estimation by Plasma Creatinine(Pcr) • In steady state Creatinine excretion = creatinine production=constant Creatinine excretion =Urine creatinine x Urine volume Filtered creatinine =GFR x Plasma creatinine As creatinine production is a function of muscle mass and remains constant Thus plasma creatinine values vary inversely with GFR GFR1/2 X 2 Pcr = GFR x Pcr = constant • A rise in Pcr almost always represents a fall in GFR
In case 4 ,serum creatinine increased from from 1 to 2 mg/dl and remained at that level, his 24urine creatinine will remain the same • Another example :70 kg man with serum creat. of 1 mg/dl and GFR of 100 ml/min was excreting 1500 mg creatinine/day,if you remove his one kidney , next day his GFR will be 50ml/min,urine creatinine excretion will be 750 mg /day.Over the next few days creatinine will accumulate in the blood and level will increase to 2 mg /dl and thus filtered and excreted amount will be the same
Summary • How to evaluate a patient with renal disease • How to interpret u/a,urine protein to creatinine ratios • Interpretation of urea nitrogen and creatinine ratios • Estimation and measurement of GFR& to see when a patient would need renal replacement therapy • Interpret urine indices in evaluation of various causes of ARF