Download
1 / 47
470 likes | 640 Views
Rational Dosing: The Use of Plasma Concentrations vs. Tissue Concentrations Hartmut Derendorf, PhD University of Florida. Drug Delivery Pharmacokinetics Pharmacodynamics. ?. Biopharmaceutics. ?. PK-PD-Modelling. Pharmacokinetics conc. vs time. Pharmacodynamics conc. vs effect. 0.4.

E N D
Rational Dosing: The Use of Plasma Concentrations vs. Tissue Concentrations Hartmut Derendorf, PhD University of Florida
Drug Delivery Pharmacokinetics Pharmacodynamics ? Biopharmaceutics ? PK-PD-Modelling
Pharmacokinetics conc. vs time Pharmacodynamics conc. vs effect 0.4 1 Effect Conc. 0.0 0 0 25 Conc (log) Time 10 -4 10 -3 PK/PD effect vs time 1 Effect 0 0 25 Time
16 • Time above MIC • AUC above MIC • Cmax/MIC • AUC24/MIC (AUIC) Cmax AUC > MIC 12 8 Concentration (µg/mL) MIC 4 0 24 12 0 6 18 Time (hours) t > MIC
FDA Bioequivalence Definition „ ... rate and extent … and becomes available at the site of action.“
FDA Guidance for Industry 1997 Part IV „Clinical Issues, Pharmacokinetics“ „... Pharmacodynamics should include relating drug concentrationsat the site of actionto the in vitro susceptibilty of the target microorganism.“
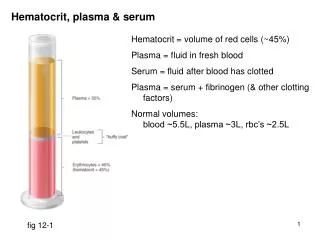
vascular space extravascular space binding to extracellular biological material plasma protein binding blood cell binding, diffusion into blood cells, binding to intracellular biological material tissue cell binding, diffusion into tissue cells, binding to intracellular biological material
Only the free, non-bound drug can be pharmacologically active Hence, total drug concentrations (“tissue levels”) should not be related to pharmacological activity From a pharmacological and clinical point of view, free tissue levels are most significant with respect to therapeutic outcome Significance of free tissue levels
Experimental Determination of Free Tissue Concentrations • Skin Blister Studies • Microdialysis
Skin Blister Kiistala (1968)
Skin Blister Kiistala (1968)
Ampicillin Cloxacillin Serum Free blister fluid
Microdialysis Dialysate Perfusate (Ringer’s) Tissue
Perfusate Dialysate Interstitium Capillary Cell
Dialysate Cout Perfusate Cin Tissue CT No net flux method If Cin > CT, then Cout < Cin If Cin < CT, then Cout > Cin
No Net Flux Method n = 4 Recovery: 37 ± 5 %
concentration [µg/ml] time [min] Piperacillin
Ceftriaxone 50 mg/kg concentration [µg/ml] time [min]
concentration [µg/ml] time [min] Ceftriaxone 100 mg/kg
FDA Draft-Guidance for Industry (1997) Providing Clinical Evidence of Effectiveness for Human Drug and Biological Products New Dosage Form of a Previously Studied Drug In some cases, modified release dosage forms may be approved on the basis of pharmacokinetic data linking the new dosage form from a previously studied immediate-release dosage form. Because the pharmacokinetic patterns of controlled-release and immediate release dosage forms are not identical, it is generally important to have some understanding of the relationship of blood concentration to response to extrapolate to the new dosage form.
ExampleDevelopment of an Oral Sustained Release Formulation for Cefaclor
Plasma Cf muscle Cf lung Cefaclor in RatsTotal plasma and free tissue levels 50 mg/kg 75 mg/kg
Microdialysis can be used to determine free cefaclor concentrations in muscle and lung tissue. Free concentrations of cefaclor in both lung and muscle tissue have almost identical profiles and are lower than the respective free plasma concentrations. Since unbound concentrations in muscle and lungs are equal in rats, Cf,muscle may be used as an estimate of Cf,lung in humans. Conclusions - Rats
12 healthy male human volunteers PO Doses: 500 mg IR (immediate release) 500 mg MR (modified release) 750 mg MR (modified release) Tissue: muscle Total sampling time: 12 hours microdialysis every 20 minutes Human study
500 mg IR Plasma and free tissue levels n = 12 (means +/- S.D.) total plasma concentrations free tissue concentrations
Plasma and free tissue levels 500 mg MR 750 mg MR n = 12 (means +/- S.D.) total plasma concentrations free tissue concentrations
Oral absorption of cefaclor can be sustained, but only to about 3h due to the presence of an absorption window Relative bioavailability of the modified release product is approximately 80% Microdialysis can be used to determine free cefaclor concentrations in human muscle tissue. Free concentrations of cefaclor in muscle tissue are lower than respective free plasma concentrations. Conclusions - Humans
Pharmacodynamics • in vitro studies • steady state • dilution models • diffusion models • animal studies • clinical studies
MIC The Current Paradigm MIC is a well established laboratory parameter routinely determined in microbiology MIC is by far the most common pharmacodynamic parameter for anti-infective agents Most PK/PD-approaches for anti-infectives are based on MIC (e.g. AUIC, t>MIC, Cmax/MIC) Drug concentrations are compared to MIC to make dosing decisions
Dilution Filter 1) Inoculum 2) Dose 3) Sample Kill Curves
PK-PD Model Maximum Growth Rate Constant k Maximum Killing Rate Constant k-kmax Initially, bacteria are in log growth phase
Single Dose Piperacillin vs. E. coli
Betalactam antibiotics kill time-dependent Piperacillin vs. E. coli 2g q4h 4g q8h
A suitable PK/PD model was successfully applied to link different cefaclor dosing regimens to their respective anti-infective activity. Using PK/PD, different dosing regimens can be compared taking into account the therapeutically active concentrations at the site of action. The results show that in spite of a 78-84% relative bioavailability 500 mg MR bid are equivalent to 500 mg IR tid. Furthermore, the same total daily dose (1.5 g) is more effective when given in a sustained way: 750 mg MR bid is more effective than 500 mg IR tid. ConclusionsCefaclor-Study
Comparison of Emax-model vs. MIC Emax-model is two-dimensional (Emax, EC50) whereas MIC is mono-dimensional. Emax-model allows for gradual changes in pharmacodynamic activity whereas MIC is a threshold value. Emax-model can be integrated in PK-PD models to characterize the complete effect-time-relationship whereas MIC can only be used in integrated models (AUIC, t>MIC). Emax-model is more complex than MIC. However, today’s computer software can handle this with ease. Emax-model allows for more differentiated dose recommendation based on microbiological data than MIC.
Conclusion The free (unbound)concentration of the drug at the receptor site should be used in PK/PD correlations to make prediction for pharmacological activity
Conclusions • Simple comparisons of serum concentrations and MICare not sufficient for proper evaluation of antibiotic agents and their dosing schemes • Protein binding and tissue distribution are critical pharmacokinetic properties that need to be considered • Pharmacodynamic kill curves can provide more detailed information about the pharmacodynamics than MICs
Acknowledgements Markus Müller Arno Nolting Teresa Dalla Costa Andreas Kovar Amparo de la Peña Ping Liu Kenneth Rand Alistair Webb