Download
1 / 25
250 likes | 419 Views
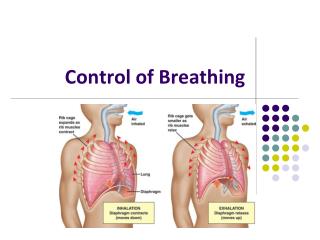
Control of Breathing . THE REGULATION OF ALVEOLARVENTILATION. The level of alveolar ventilation is driven mainly from the input of specific chemoreceptors to the central nervous system. Chemoreceptors monitor the chemical composition of body fluids.

E N D
THE REGULATION OF ALVEOLARVENTILATION • The level of alveolar ventilation is driven mainly from the input of specific chemoreceptors to the central nervous system. • Chemoreceptors monitor the chemical composition of body fluids. • In this system, there are receptors that respond to pH, PCO2, and PO2 .
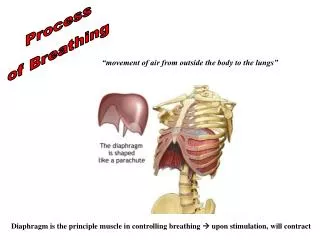
Inspiratorycenter Apneustic center • The inspiratory center controls the basic rhythm for breathing by setting the frequency of inspiration. • The inspiratory center sends its motor output to the diaphragm via the phrenic nerve. • Excites the inspiratory center in the medulla, prolonging the period of action potentials in the phrenic nerve, and thereby prolonging the contraction of the diaphragm.
Pneumotaxic Center • The pneumotaxic center (location: upper pons) turns off inspiration, limiting the burst of action potentials in the phrenic nerve. • Effect : It limits the size of the tidal volume, and it regulates the respiratory rate. • A normal breathing rhythm persists in the absence of this center.
Peripheral Chemoreceptor System for Control of Respiratory Activity—Role of Oxygen in Respiratory Control
Peripheral chempreceptors are more sensitive to PO2 • whereas the Central chemoreceptors are more sensitive to PCO2.
Acid–base Considerations • When CO2 dissolves in water, it forms carbonic acid. Although a relatively weak acid, it is produced in such prodigious quantities (>20 moles/day) that it could seriously interfere with normal tissue function if its levels were not closely monitored and regulated. • In practice, the central nervous system (CNS) maintains plasma pH within an extremely tight range (pH 7.35–7.45), in part by adjusting ventilation to hold Paco2 at around 40 mm Hg.
Causes of changes in extracellular fluid pH • Changes in pH caused by the lungs are referred to as respiratory acidosis or respiratory alkalosis. Non respiratory changes are referred to as metabolic acidosis or metabolic alkalosis. • Respiratory acidosis: Increased Paco2 results from hypoventilation, V̇A/Q̇ mismatches, or an increase in the diffusional distance between the alveolar sac and pulmonary blood supply (due to pulmonary fibrosis or edema, for example). • Respiratory alkalosis: Paco2 decreases with hyperventilation, typically because of anxiety or other emotional state. It can also result from hypoxemia precipitated by ascent to high altitude.
Decreases in arterial pH • Decreases in arterial pH cause an increase in ventilation, mediated by peripheral chemoreceptors for H+. • This effect is independent of changes in the arterial PCO2 and is mediated only by chemoreceptors in the carotid bodies (not by those in the aortic bodies).
Decreases in arterial pH • In metabolic acidosis, when there is decreased arterial pH, the peripheral chemoreceptors are stimulated directly to increase the ventilation rate (the respiratory compensation for metabolic acidosis)
Other receptors • Lung stretch receptors, • Joint and muscle receptors, • Juxtacapillary(J) receptors • Afferent impulses from baroreceptor • Higher center
Abnormal Breathing Patterns • Apneustic breathing • Biot’s breathing • Cheyne-Stokes breathing