Download
1 / 91
990 likes | 1.42k Views
Assessment of Control of Breathing, P0.1, CO2 Stimulation Test. 吳惠東. Lecture Content. Respiratory center physiology Respiratory center output chain P0.1 definition P0.1 technology Clinic application of P0.1 Respiratory physiology, Pharmacology COPD MV adjustment Weaning.

E N D
Assessment of Control of Breathing, P0.1, CO2 Stimulation Test 吳惠東
Lecture Content • Respiratory center physiology • Respiratory center output chain • P0.1 definition • P0.1 technology • Clinic application of P0.1 • Respiratory physiology, Pharmacology • COPD • MV adjustment • Weaning
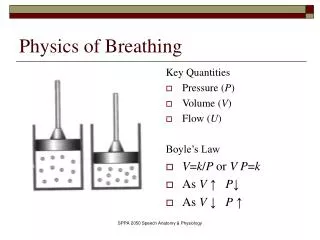
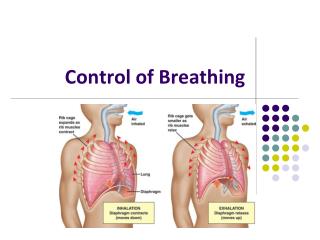
Control of breathing, Important Gas exchange in the lung can be divided into • Ventilation • Diffusion • Perfusion • Control of breathing
Control of Breathing, Passive lung • Ventilation (of lung) is a passive behavior • There is no rhythm generator (pace maker) nor respiratory muscle in the lung • All respiratory muscle are striated muscle which controlled by nerve, the striated muscle without autonomic activity in the usual
Respiratory Center • Sensor input • Central, peripheral • Chemorecepotrs (O2, CO2, pH? ), stretch receptor, irritant receptors, J receptors, …. • Voluntary, involuntary • Rhythm activation and integration • Motor output
Respiratory Central Network • Respiratory center is not a single cell, not a single group of cells, but a network of many groups of neuron • Respiratory rhythm is generated by a network of medullar neurons and transmitted by nerves to active respiratory muscle • Rhythm generator • On-switch and off-switch of inspiratory and expiratory activity • Pattern generator • Shapes the activity patterns of neuron
Respiratory Center • Central respiratory rhythm: oscillating network in ventrolateral reticular formation of the brainstem, “pre-Botzinger Complex” • Respiratory phase: Inspiration, post inspiration (E-2), expiration (active exhalation), late expiration (passive expiration), .. • Many neurons involved • Pre-inspiratory, early-inspiratory, throughout-inspiratory, late-inspiratory, postinspiratory, expiratory,…
Respiratory Center Neuron Transmitter • Neurons synaptic activation mediated by glutamate • NMDA, AMPA, • Most inhibitory mediated synaptic by GABA (Cl channel) • Early- and postinspiratory is glycinergic
Respiratory Center Neuron Activity • Both excitation and inhibition • Inspiration starts when early- and throughout-inspiratory neurons are released from postsynaptic inhibition • The inspiratory ramp activity is also transmitted to late-inspiratory neurons • The discharge of late-inspiratory neurons inhibit early-inspiratory neuron
Respiratory Drive Index • Tidal volume, respiratory frequency • Minute ventilation: marked variation, lung mechanism dependent • Measurement of nerve or muscle electrical activity • Mean inspiratory flow rate (MIF, VT/Ti) • Inspiratory time fraction (Ti/Ttot) • Mouth occlusion pressure
Measurement of Respiratory Neuron Output CNS electrode Too invasive Phrenic N activity Invasive, Difficult to compare Diaphragm muscle Noise, Complicate activity Difficult to compare Ventilation Simple to measurement Indirect method Noninvasive Affected by chest Measure total output mechanism and muscle O2 cost of Noninvasive Indirect method breathing Measure total output Difficult to measure accurate
Respiratory pattern generation • Classically, breathing pattern is analyzed by respiratory frequency (f) and tidal volume (VT) • Animal studies suggests the respiratory center output is controlled by driving (force) and duty cycle • Ventilation = Flow (amplitude) * Time • VE = VT x f = (VT/Ti) * (Ti/Ttot) * 60 (l/min) • Ti/Ttot: inspiratory duty ratio • VT/Ti: mean inspiratory flow rate, an index of the intensity of the driving • VT/Ti and Ti/Ttot is interpreted as drive and timing components of ventilation which are somewhat controlled independently.
Time: Ti, Ti/Ttot Flow: MIF Time Control versus Flow Control
Mouth Occlusion Pressure • Occluded mouth (airway) pressure change after 100 msec initial inspiration • P0.1 • Assume mouth pressure equal to alveolar pressure in zero flow condition, by occluded airway • Although negative in nature, P0.1 values are usually reported in positive units (cmH2O) • It presents as the force output of respiratory center
Termination of P0.1 • Mouth occlusion pressure • Airway occlusion pressure • P0.1 , P100
Other express of occlusion pressure • Maximal rate of change in mouth pressure dP/dtmax • Maximal rate of change in mouth pressure in first 100msce • P0.1eso • Peso max in non-occlusion method
Characteristics of P0.1 (I) • Respiratory muscle contraction in occluded airway (no flow, iso-volume, isometric constriction) • Under isometric condition the force produced by a muscle changes proportionally to its electrical activity • Less influenced by lung mechanism changes • Correlate to respiratory center activity, phrenic nerve electrical activity and diaphragm force output
Characteristics of P0.1 (II) • No pressure loss due to resistance or elastance • Index of respiratory center output • Relatively regardless of the subject's lung condition • Till severe respiratory muscle weakness, P0.1 is little changed with muscle weakness • Before subject recognizes the occlusion and reacts to it (100 msec), less conscious dependent
Normal value • P0.1 (non stress): 0.98 +/- 0.48; usually less than 2 • P0.1/PCO2: slope 0.6 (SEE 0.11)
Tips of P0.1 measurement • The tester unknowns the occlusion (occlusion time less than 0.2sec, without conscious interference) • Airway rapid occluded before inspiration • Adequate occlusion time • Complete occlusion • The lung volume (FRC, EELV) are not significant changed during testing
Factors Influencing Measurement of Occlusion Pressure • Alteration in end-expiratory lung volume • Time constant of the respiratory system • Alteration in muscle length and velocity • Chest wall distortion • Expiratory muscle activity • Shape of the driving pressure wave • Pressure-flow phase lag
Factors Influencing Measurement of Occlusion Pressure • Alternation in end-expiratory lung volume • Time constant of respiratory system • Alteration in muscle length and velocity • Chest wall distortion • Expiratory muscle activity • Shape of the driving pressure wave • Pressure-flow phase lags • Expiratory pause • P0.1 measure the onset of mechanic but not neural inspiration
Airway Occlusion Recording No flow No -Occlusion Occlusion
Application of P0.1 • Central respiratory driving physiologic study • Assess the effect of drugs to respiratory center • Assess the effect of diseases to respiratory center • Adjusting mechanical ventilation setting • Predict the weaning outcome
Conditions Influence P0.1 • P0.1 increase in • Increase ventilatory load • Asthma • Breathing viscous gas mixture • Even blood gas is held constant • Respiratory center stimulant, anxiety • P0.1 depressed by • Tranquilizers • Alcohol • Central nerve system hypoxia
P0.1 and COPD (I) • Ventilation (tidal volume, minute ventilation) is significantly influenced by flow resistance, compliance and respiratory muscle strength • Measurement of diaphragmatic EMG, oxygen cost of breathing and inspiratory mechanical work rate have been used but they are technically complex, time consumption and nonstandardized
P0.1 and COPD (II) • P0.1 at rest are either normal or increased in chronic muscle weakness (Begin, ARRD 1982) • In COPD, high values and electromyographic sign indicate impending diaphragmatic fatigue • No correlation between P0.1 and ABG • In normal healthy individuals p0.1 values of 6-8 cmH2O can only be obtained with a maximal voluntary ventilation (MVV) between 50 - 70 l/m