Download
1 / 67
670 likes | 787 Views
Hepatitis C: Boomers at Risk Diagnosis and Treatment Outcomes. Richard K. Sterling, MD, MSc, FACP, FACG VCU Hepatology Professor of Medicine Chief, Section of Hepatology Fellowship Director, Transplant Hepatology Virginia Commonwealth University Richmond, VA.

E N D
Hepatitis C: Boomers at RiskDiagnosis and Treatment Outcomes Richard K. Sterling, MD, MSc, FACP, FACG VCU Hepatology Professor of Medicine Chief, Section of Hepatology Fellowship Director, Transplant Hepatology Virginia Commonwealth University Richmond, VA
Conflicts of Interest in the last 12 months • Advisory Board • Roche/Genentech, Merck, Vertex, Bayer, Salix, BMS, Abbott, Gilead • Research support • Roche/Genetech, Merck, Bayer, Gilead, Abbott, Boehringer Ingelheim, Vertex, BMS
Goals of Discussion • Epidemiology of HCV • Populations to test (Boomers and those with risks) • Approach to patient (Diagnosis and testing) • Treatment (past, present, future) • Impact of treatment • Future (at least as I see it)
Liver failure Other organs Stop working Liver cancer Some basic facts about liver disease DEATH Chronic Liver disease cirrhosis LIVER TRANSPLANT ~ 8-10 million Americans affected
Global epidemiology of hepatitis C virus infection: New estimates of age‐specific antibody to HCV seroprevalence HepatologyVolume 57, Issue 4, pages 1333-1342, 4 FEB 2013 DOI: 10.1002/hep.26141http://onlinelibrary.wiley.com/doi/10.1002/hep.26141/full#fig3
Hepatitis C • HCVis the leading cause of end stage liver disease and indication for liver transplant. • HCV is an important risk factor for diabetes and also increases the risk of heart disease. • HCV is a potentially curable disease • Risk factors: • Birth cohort: Born between 1945-1965 • risk factors: • Blood and blood product transfusion • IVDA • Cocaine snorting • Multiple sex partners with unprotected sex
Time is critical • The average age of an HCV-infected patient is approximately 55 yrs • Perhaps 40% have cirrhosis • 10,000-15,000 die each year and is increasing • Only 25-30% of HCV patients have been diagnosed • Only 11% have been treated
The growing burden of viral hepatitis in the United States Annals Int Med 2012
How much does viral hepatitis contribute to cirrhosis and HCC
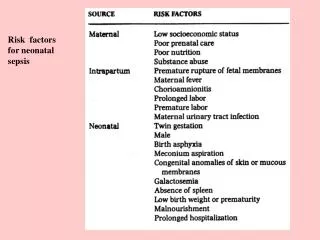
The burden of end-stage liver disease N=104 cirrhotic subjects Veterans and non-vets equally affected MELD and HE drives caregiver burden Bajaj et al
Why is the situation particularly tragic ? • Risk factors for viral hepatitis are well known • A highly effective vaccine for hepatitis A and B exists • Tests to diagnose the disease are available and are being improved upon- and should allow point of care testing • Highly effective treatments for both hepatitis B and C are available and getting better
How to prevent hepatitis C? • Safe blood supply • Intravenous drug users • Iatrogenic spread (improve health care associated outbreaks) • ? Safe sex methods
What can we do? • Detect early and prevent disease progression • Identify those with clinically silent but serious disease who are at greatest risk for morbidity and mortality
Birth Cohort Screening • Baby boomers: birth between 1945-65 • Risk factor based screening below that • Well known prevalence and risk factors • Contribution to burden of disease well established • Highly sensitive diagnostic tests available • Effective therapy is available • Treatment reduces mortality and morbidity CDC guidelines 2012 Despite the USPSTF recommending that only high risk individuals be tested (blood transfusion prior 1992, illicit drug use, increased ALT), most, if not all others (AASLD, CDC, ACG, AGA, VAHA, NIH, ISDA, IOM) endorse birth cohort screening regardless of risk factors (Edlin BR. Hepatology 2013;57:1644-1650)
Impact of timing and prioritzation for treatment on cost effectiveness of birth cohort screening Age McEwan et al, Hepatology. 2013 Feb 6. doi: 10.1002/hep.26304.
More quality adjusted life years saved with prioritization for Rx for more advanced disease McEwan et al, Hepatology. 2013 Feb 6. doi: 10.1002/hep.26304.
Evaluation of HCV HCV Ab + HCV RNA and Genotype - + Liver Enzymes CBC with Plt HBV sAg/sAb/cAb HAV IgG HIV ANA + Repeat HCV RNA - Avoid alcohol Counsel on household and sex Vaccinate for HAV and HBV Avoid raw shell fish Resolved HCV Assess severity of disease (liver biopsy or non-invasive test) Assess for treatment (May require referral)
How to identify clinically silent but significant disease in your clinic Know the epidemiology of disease in your area Evaluate risk factors: Alcohol history Body weight and type 2 diabetes High risk behavior for viral hepatitis Abnormal liver enzymes Use of simple methods to identify those with fibrosis
Ability of abnormal ALT to detect chronic hepatitis Prati et al, Ann Intern Med, 2002; 137:1-9
Strategies to identify those with serious but silent disease • AST: ALT > 1 • Flip in AST: ALT ratio • Decreasing platelet count • Other non-invasive markers • ELF score • Fibrotest (Fibrosure) • Fibroscan • FIB4 • APRI
Past HCV Therapy (2001-2011)PegIFN + RVN % SVR % Rx 10% 60% GT 1 and 4 GT 2 and 3
Favorable Genotype 2 and 3 HCV RNA < 400,000 IU/ml Mild fibrosis (F0-F2) Non-African American Age < 40 IL28B CC Adherence RVR cEVR Unfavorable Genotype 1 HCV RNA > 400,000 IU/ml Advanced fibrosis (F3-F4) African American Age > 40 Steatosis Insulin Resistance Increased BMI IL28B CT or TT Dose reduction > 60% Non-adherence Predictor of Response with PEG/R
IL28-B POLYMORPHISMIMPACT ON SVR D Ge et al. Nature 2009; 461:399-401.
IL28-B POLYMORPHISM AND SVRIMPACT OF RACE AND ETHNICITY Asians Caucasians Hispanics African Americans D Ge et al. Nature 2009; 461:399-401.
HCV Polyprotein Processing and Viral Protein Function Complex Inhibitor McGovern B, Abu Dayyeh B, and Chung RT. Hepatology. 2008; 48:1700-12
ADVANCE: Telaprevir with Response Guided Therapy in naïve HCV-1eRVR = HCV RNA(-) @W4,12: Yes 24W, No 48W TPV 750 mg q8h; PEG-2a; WB RBV P <0.0001 100 P < 0.0001 75 80 69 60 44 SVR (%) 40 20 0 PegIFN/RBV + Placebo 48w (n=361) TPV 12w+ PegIFN/RBV RGT (n=363) TPV 8w+ PegIFN/RBV RGT (n=364) eRVR, % Relapse, % DC rash, T or Pl/all % DC any AE,% Jacobson I et al, NEJM 2011;364:2405-16
ILLUMINATE: Randomized trial of short vs. long duration Rx after eRVR GT 1, Txnaive (N=540) Peg2a /WB RBV/TPV x 12 wks Wk 4, 12 HCV RNA (-) 65.2% (n=352) Randomize +12 wks P/R (n=162) +36 wks P/R (n=160) SVR 92% SVR 87% • met noninferiority criteria • A truncated PEG/RBV/TPV regimen preserves high rates of SVR following eRVR Sherman K et al, AASLD 2010; abstract LB-2
HCV TREATMENT FOR NAIVEStandard of Care- Present Confirm HCV Present Determine VL and Genotype Evaluate Severity (Histology) Evaluate Contraindications to Rx Genotype 1 (or 4) Genotype 2 or 3 DAA +Peg IFN alfa 2a or 2b + ribavirin (wt. based) for 48 wks Peg IFN alfa 2a or 2b + ribavirin 800 mg/qd for 24 wks RGT or Futility Early d/c SVR 70-80% SVR 65-75% Pooled SVR 70-80%
Response Guided Therapy with Boceprevirnon-cirrhotic HCV RNA Undetectable < 100 IU/mL Undetectable Lead in PR BOC + P + R eRVR, stop at week 28 0 4 8 12 24 28 36 48 Detectable < 100 IU/mL Undetectable No RVR PR PR BOC + P + R 0 4 8 12 24 28 36 48 Stop If HCV RNA > 100 IU/mL
Response Guided Therapy with Telaprevirnon-cirrhotic naïve or experienced relapsers HCV RNA Undetectable Undetectable Undetectable T + P + R P+R eRVR, stop at week 24 0 4 8 12 24 28 36 48 Detectable < 1000 IU/mL Undetectable No RVR PR T + P + R 0 4 8 12 24 28 36 48 Stop If HCV RNA >1000 IU/mL
Treatment of Null Responders and Cirrhotics HCV RNA Undetectable < 100 IU/mL Undetectable Lead in PR BOC + P + R 0 4 8 12 24 36 48 HCV RNA Undetectable Undetectable Undetectable T + P + R P+R 0 4 8 12 24 28 36 48
Monitoring HCV RNA • Package inserts for TVR and BOC specific different time points during therapy. • TVR weeks 4, 12, and 24 • BOC weeks 8, 12 and 24 • Different labs use different assays. • Different thresholds for using RGT. • TVR week 4 1000 IU/mL • BOC week 8 100 IU/mL • Different thresholds for defining futility.
Perceived Barriers to HCV Tx • Patient Related • Side effects • Cost • Success rate • Duration • Stigmata of Tx • Experience of provider • Wants to wait for better Tx • Provider Related • Lack of experience • Lack of office infrastructure • Poor reimbursement • Lack of referral to experienced provider • Government Related • Restrictions to Tx • Funds to Tx • Lack of promotion • Payer Related • Cost of meds • Restricting coverage or providers • Excessive paper work • Excessive requirements of testing McGowan et al. Hepatology 2013;57:1325-1332
Caution in cirrhosisCUPIC TREATMENT EXPERIENCED Genotype 1- Cirrhotics SVR 12 • National Registry-France • N= 674 (295 TVR; 190 BOC) • Patients treated with DAA/PegIFN/riba by choice of clinician • All patients Child A • Results • SAE 51-54% • Death 1.6% (BOC) 2.4% (TVR) • Infection 2.5-8.8% • Hepatic decompensation 5% • Epo use 57-62% • Transfusion 14-18% • Predictors of Poor Outcome • Alb<3.5 • Plts < 100,000 Fontaine EASL 2013 #60
Issues Limiting Current DAA/PegIFN/Ribavirin Treatment of HCV • Inexperience of treaters • Psychiatric complications • Anemia • Neutropenia • Thrombocytopenia • Dermatologic events
TREAT OR WAIT? • What is coming? • When? • Interferon Free or With Interferon? • What Will It Cost?
Two Parallel Paths in Development • PEG-IFN/RBV + add-ons: • Triple: PI, NS5A, Nuc, NNPI, CypA, • Quad: PI+Nuc, PI+NS5A, PI+NNPI • Interferon backbone difficult/intolerable for some pts • Interferon-free combination therapy: • Strategies: PI+Nuc, PI+NS5A, PI+N5B Non-nuc Poly Inhib, Nuc+Nuc • With and without RBV
HCV TREATMENT LANDSCAPE DAAs in development Nucleotide NS5B Polymerase Inhibitors DAA Combinations Nucleoside NS5B Polymerase Inhibitors Preclinical BI Phase I Japon Tonbacco Gilead R0622 (Roche) Pharmasset Phase II Medivir (Tibotec) IDX 184 (Idenix) BI Others Vitamine D GLS9393 (GSK) Vertex Phase III Nitazoxamide (Romark) R7128 (Roche) ROCHE BMS Biocryst Abbott INX 189 (Inhibitrex) Celgosivir Filed Cyclophilin. I IFN λ (Zymogen/Novartis) Bavituximab Sofosubir Gilead) Debio025/ NIM811 (Novartis) Taribavirin (Valeant) Silibinine BMS791325 (BMS) SCY-835 Filibuvir (PFE) BMS 790052 (BMS) Telaprevir (Vertex/JJ) Boceprevir (MSD) GS9190 (Gilead) AZD-7295 (AZN) ABT267 (ABT) IDX 375 (Idenix) ACH-2928 (Acillion) Vx222 (Vertex) PPI-461 ANA598 (Anadys) MSD RG7348 (Roche) GS-5885 BI201127 (BI) Idenix719 TMC-435 (Tibotec/JJ) BI201335 (BI) ABT333 ABT072 (ABT) TMC 647055 (Tibotec) Vertex ITMN191/R7227 (Roche/Intermune) BMS 824393 (BMS) MK7009 (MSD) PPI-1301 A837093 (Abbott) BMS650032 (BMS) GSK ABT450 (ABT) EDP-239 (Enanta) VX-916 VBY-376 GS9256 (Gilead) GS9451 (Gilead) VX-759 IDX 077 (Idenix) Non Nuc NS5B Polymerase inhibitors ACH2684 (Achillion) MK5172 (MSD) VX-985 (Vertex) NS5A inhibitors IDX 079 (Idenix) VX-813 (Vertex) AVL-192 (Avila) AVL-181 (Avila) NS3/4A Protease inhibitors Adapted from Bourliere M. HepDart 2011
NEUTRINOSofasbuvir (NS5B Poly Inhib) + Peg/RVN x 12 weeksGT 1 (90%),4,5,6 Tx Naive % Lawitz NEJM 2013 N=327
MK 5172 (PI) 12 w + Peg/RVN RGTGT1, Tx naïve, no Cx % Manns EASL 2013
Faldaprevir + P/R vs. P/R RGTNS 3/4 PI (BI 201235) EASL 2013
Ledipasvir (GS 5885) + GS 9451NS5A Complex Inhibitor + Protease InhibitorGT 1 Tx Naïve, IL28B CC, no Cirrhosis % EASL 2013
What about interferon free? Holy Grail
SOFOSBUVIR (GS 7977 NS5B Nuc Pol Inhib)Genotypes 1/2,3 Genotype 1 Genotype 2/3 Gane et al., NEJM, 2013
FISSIONSofosbuvir/RVN (12w) vs. PEG/RVN (24w) GT2/3 Treatment Naive Lawitz et al. NEJM 2013
FUSIONGT2/3 Tx ExperiencedSofosbuvir + RVN (12 vs. 16 weeks) % Jacobson NEJM 2013