Download
1 / 31
350 likes | 1.34k Views
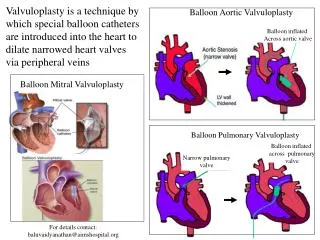
Peter C. Block M.D. Andreas Gruentzig Cardiovascular Center Emory University. Balloon Aortic Valvuloplasty. AATS Sept. 2005.

E N D
Peter C. Block M.D. Andreas Gruentzig Cardiovascular Center Emory University Balloon Aortic Valvuloplasty AATS Sept. 2005
“When it is considered how narrow the opening is, which these constrictions leave, it is difficult to conceive how such an organic derangement can continue for years. It is evident, if such an obstacle to the circulation were suddenly introduced into a healthy subject, death would immediately follow: but as these obstacles are slowly formed, the circulation is gradually impeded and nature seems in some measure to be habituated to such a perversion of her laws.” J. N. Corvisart 1803
ACC GuidelinesAortic Stenosis “In the vast majority of adults, AVR is the only effective treatment for severe AS……. Although there is some lack of agreement about optimal timing of surgery, particularly in asymptomatic patients…….” • Bonow et al. ACC/AHA task Force Report
Balloon Valvuloplasty:The History • 1950’s Intraoperative dilatation for valve conservation • 1982 Pulmonary Valve in Children • - Kan • - Pepine • 1983 Hypoplastic PV and PA’s – Lock • Coarctation – Lock • 1984 Aortic stenosis in Children – Lababidi • 1983 Mitral stenosis Inoue • 1985 Acquired Aortic stenosis in 3 pts– Cribier • 1987 Aortic stenosis in Children - Choy • 1987 Cribier - 92pts and Block - 55pts • 1986 Mansfield Registry • 1987 NHLBI Registry
What is the role of Balloon Aortic Valvuloplasty in 2005? • Neonatal, childhood and adolescent applications are well established. • 2) Fetal application remains experimental. • 3) The rare adult with AS
Aortic Valve ReplacementNew York State 2002 • 77,075 Heart Operations • 19,057 Valve operations • 4943 Isolated Aortic Valve Replacements • Mortality 3.54% • 4704 Aortic Valve Replacement with CABG • Mortality 6.27%
Aortic StenosisSurvival without Intervention Ross J. Circ 1968; 37, Suppl V Carabello, B. A. N Engl J Med 2002;346:677-682 O’Keefe et el. 1987.
Balloon Aortic ValvuloplastyMajor Series • Mansfield Scientific Registry, n = 492 • NHLBI Registry, n = 674 • Cribier (French Registry), n = 406 • Block , n = 375 • Safian , n = 170 • Lieberman , n = 165 • Lewin , n = 125 • Ferguson , n = 73
Balloon Aortic ValvuloplastyAcute Outcome“Success” ? • Mansfield Registry • 87% Success - i.e. alive, no AVR, a significant Δ AVA • NHLBI • 95% • Kuntz et al • 93% “In absence of data correlating final AVA to clinical response, and in the difficulty in estimating AVA …… Any definition of success is … arbitary” - Bashore et al
Balloon Aortic ValvuloplastyAcute Hemodynamic Results 674 pts in NHLBI Registry Circ 1991;84:2383-2397
Balloon Aortic ValvuloplastyAcute Hemodynamic ResultsValve Area AVA increased 0.5 ±0.2 to 0.8 ±0.3 cm2 Range 0.1 – 1.4 to 0.1 – 3.4 cm2 • 77%ΔAVA < 0.4 cm2 • 13%ΔAVA 0 cm2 • AVAF≥ 1cm2 in only 29% “Start with AS and end with AS” NHLBI. n = 674 Circ 1991;84:2383-2397
Balloon Aortic ValvuloplastyEffect of Procedural variables “..the optimal technique . . . . not yet defined” n = 492; < or > 20mm < or > 30 sec McKay 1991 JACC
Balloon Aortic Valvuloplasty30 Day Functional Status NYHA Functional Class (364 improved) Functional Class Score (257 improved) 484 Survivors from NHLBI Registry
Balloon Aortic ValvuloplastyHemodynamic Follow-upMansfield Registry Post BAV 6 month f/u * n = 95 n = 95 AVA Baseline - cm2 AVA Baseline - cm2 6.2 ±3.3 mnths Bashore JACC 1991:1188
Balloon Aortic ValvuloplastyHemodynamic Follow-up 6.2 ±3.3 mnths n = 95 Mansfield Registry Bashore JACC 1991:1188
Balloon Aortic Valvuloplasty Complications - %
Balloon Aortic ValvuloplastyArteriotomy management • Manual, C-clamp or Femostop • Suture closure • Post procedure with 10F sheath • Preclose with 6 or 8F devices • Feldman,Michaels, Marchant & Solomon: successful closure with no complications
Balloon Aortic Valvuloplasty Mortality - % * Procedural
Balloon Aortic ValvuloplastyPredictors of 30 day Mortality Variables identified in multivariate analysis
Balloon Aortic ValvuloplastyClinical Follow-up Mansfield Registry Data 6.2 ±3.3 mnths n = 95 Bashore JACC 1991:1188
Balloon Aortic ValvuloplastyLong Term Follow up Months Kuntz R NEJM 1991;325:17
Balloon Aortic ValvuloplastyWhy such poor outcomes ? • The procedure • Fracture of calcific nodules • Commissural splitting • Annular stretching The patient Medical Co-morbidities Coronary Artery Disease ≥50% of patients Inadequate residual valve area < 1 cm2 in most patients post procedure
Aortic Stenosis Recommendations for Aortic Balloon Valvotomy in Adults With Aortic Stenosis Bonow et al. 1998 ACC/AHA Task Force
Balloon Aortic Valvuloplasty? • Benefits • Yes, but transient • Risks • Yes • Alternatives • AVR • Alters natural history but also carries risk • Percutaneous AVR ? • The future? • The only role for BAV ?
But wait…… Balloon Aortic Valvuloplasty (may) will be necessary again….. as a preliminary to Perc. AVR
Take home messages: • BAV may hold some valuable lessons for the future of Rx of aortic stenosis • BAV may still be needed to help rearrange/split/move Ca++ • BAV may be needed to allow passage of PAVR devices • In the desperately ill pt. BAV may be lifesaving and allow further therapeutic options