Download
1 / 71
710 likes | 728 Views
Learn about a 60-year-old man with head and spine injuries from a motorcycle accident. Understand symptoms, mechanisms of injury, and assessment techniques. Discover the importance of recognizing secondary complications and providing emergency medical care.

E N D
Chapter 29 Injuries to the Head and Spine
Case History You respond to a 60-year-old man who fell while riding a motorcycle without a helmet. He has a contusion on the left side of his forehead and fluid leaking from his nose, mouth, and ears. He is verbally combative but cannot move his upper and lower extremities.
Skeletal System • Provides structure and support • Protects vital organs • Allows movement, in conjunction with muscles
Nerve Cells and Pressure • Nerve cells are very sensitive to pressure. • When pressure is applied to nerve cells, function becomes compromised. • Determinants of injury from pressure: • The amount of pressure applied on nerve • The period of time over which it is applied
Lateral Bending • Distraction • Pulling apart of the spine • Example: Hanging
High Index of Suspicion for Spinal Injury • Motor vehicle crashes • Pedestrian vs. vehicle collisions • Falls • Blunt trauma
High Index of Suspicion for Spinal Injury • Penetrating trauma to head, neck, or torso • Motorcycle crashes • Hangings • Diving accidents • Unconscious trauma victims
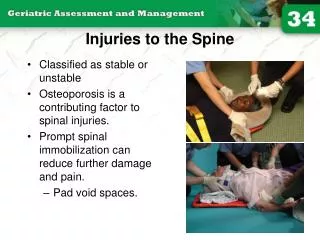
Spinal Injuries –Signs and Symptoms • Tenderness in the area of injury • Pain associated with moving • Do not ask the patient to move to try to elicit a pain response. • Do not move the patient to test for a pain response. • Tell the patient not to move while you are asking questions. • Normal function does not rule out spinal injury.
Spinal Injuries –Signs and Symptoms • Pain independent of movement or palpation • Along spinal column • Lower legs • May be intermittent • Obvious deformity of the spine on palpation • Soft tissue injuries associated with trauma • From head and neck to cervical spine • Shoulders, back, or abdomen (thoracic, lumbar region) • Lower extremities (lumbar, sacral region)
Loss of Sensation and Function Below Level of Injury • Loss of sensation and paralysis • C4: clavicles • T4: nipple line • T10: navel • L1: groin • Level of injury – respiratory paralysis • Above C3, complete paralysis/respiratory arrest • Below C5, intercostals and abdominals, diaphragmatic breathing only • Upper or lower extremities • Incontinence
Assessment of Spine-Injured Responsive Patient • Mechanism of injury • Questions to ask • Does your neck or back hurt? • What happened? • Where does it hurt? • Can you move your hands and feet? • Can you feel me touching your fingers? • Can you feel me touching your toes?
Assessment of Spine-Injured Unresponsive Patient • Mechanism of injury • Initial assessment • Inspect for • Contusions • Deformities • Lacerations • Punctures/penetrations • Swelling
Assessment of Spine-Injured Unresponsive Patient • Palpate for areas of tenderness or deformity. • Obtain information from others. • Mechanism of injury • Mental status
Complications • Inadequate breathing effort • Prepare for positive-pressure ventilation. • Maintain manual inline stabilization. • Paralysis
Emergency Medical Care • Body substance isolation • Determined by presenting problem • Goggles • Gloves • Mask • Gown
Critically Injured Patient • Perform a rapid extrication. • Bring body into alignment. • Transfer to long board without short spine board. • Transport immediately.
Injuries to the Head –Structural Specific sections of the brain are injured. • Brain lacerations • Brain contusions • Blockage of vessels (stroke) • Injuries can be traumatic or nontraumatic.
Structural Injuries –Signs and Symptoms • Result in localized findings (unilateral) • Unequal pupils • One-sided paralysis • One-sided sensory loss
Metabolic Injuries • Interruption of energy needed for cell life • Poisoning • Hypoxia • Low blood sugar
Metabolic Injuries – Signs and Symptoms • Symmetrical findings • General signs of CNS dysfunction
Secondary Complications of Brain Injury • Hypoxia • Hypotension • Hypoglycemia • Infections • Increased intracranial pressure
Significance of Secondary Complications • Occur with direct brain injury • Aggravate brain function • Management is important to overall care. • Treatment prevents further injury to the brain.
Injuries to the Brain and Skull • Most common cause of traumatic death • May be immediate • May occur over time • Rapid recognition and management is key. • Access to surgical intervention is critical. • Immobilization, airway, and ventilation • Key to prehospital care
Injuries to the Brain and Skull • Scalp • Skull fracture • Concussion • Increased intracranial pressure • Epidural hematoma • Subdural hematoma
Related Nontraumatic Conditions • Clots or hemorrhage • Nontraumatic brain injuries • Can be a cause of altered mental status • Signs and symptoms parallel those of traumatic injuries • No evidence of trauma • Lack of mechanism of injury
Skull Injury –Signs and Symptoms • Mechanism of trauma • Scalp injuries • Contusions • Lacerations • Hematomas • Deformity to the skull
Skull Injury –Signs and Symptoms • Blood or fluid leakage from the ears or nose • Bruising around the eyes • Bruising behind the ears (mastoid process)
Concussion • Transient loss of consciousness or neurologic function • Many degrees of injury • Least severe • Momentary loss of function immediately after injury • Short period of confusion
Concussion –More Severe • Brain contusion • Vision loss • Paralysis • Sensory deficits
Signs of Increased Intracranial Pressure • Conscious patients • Headaches • Nausea • Vomiting (sometimes projectile) • Alterations in consciousness may occur • Sleepy • Responds to verbal stimuli • Responds to painful stimuli • Unresponsive
Signs of Increased Intracranial Pressure in Children • Drowsiness, nausea, vomiting • Even after minor head injury • Worsening may be due to • Hypoxia • Hypotension • Other causes
Eye and Motor Findings • Unilaterally dilated pupil • May not constrict with light • Eyelid may droop • Unilateral weakness, paralysis, sensory loss, or a combination may be seen. • As pressure increases, motor and sensory findings may affect both sides. • With further deterioration, abnormal postures or positions may be seen. • Eventual flaccidity
Respirations • Abnormal respiratory patterns
Pulse and Blood Pressure • Late sign of increased intracranial pressure • Pulse slows. • Blood pressure increases.
Epidural Hematoma • Requires rapid recognition and early surgical intervention • Usually presents with short period of unconsciousness after blunt trauma to head, followed by lucid interval, then decrease in LOC • Blown pupil on side of injury • Weakness and sensory impairment on opposite side of body • Abnormal respiratory pattern • Abnormal posturing • Possible high blood pressure and slow pulse • If left untreated, death occurs.