Download
1 / 30
310 likes | 540 Views
Non- neoplastic disorders of salivary glands. Assoc. Professor Jan Laco, MD, PhD. Congenital disorders. very rare agenesis congenital polycystic degeneration of parotis girls, childhood, fluctuating swelling congenital sialectasia of parotis anomalies of main excretory ducts

E N D
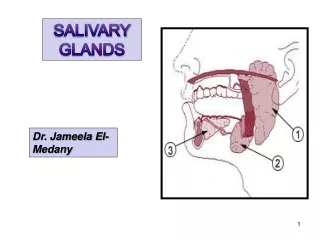
Non-neoplasticdisordersof salivary glands Assoc. Professor Jan Laco, MD, PhD
Congenitaldisorders • very rare • agenesis • congenital polycystic degeneration of parotis • girls, childhood, fluctuating swelling • congenital sialectasia of parotis • anomalies of main excretory ducts • accessory gland • ectopic gland (Stafne bone cavity)
Acutebacterialsialadenitis • streptococci A, staphylococci, anaerobs • routes • ascendent from oral cavity (sialodochitis sialadenitis) • hematogennous (in sepsis) • lymphogennous (from intra- and peri-parotid LN) • predisposition • poor oral hygiene , inflammation in oral cavity, hyposialia • drugs: tricyclic antidepressants • clinically • painful swelling, reddening f skin, pus discharge from duct • Mi: acute purulent sialadenitis + abscesses
Acutebacterialsialadenitis • treatment: ATB, event. absces drainage • CAVE!!! • dehydration, cachexia, terminal status in malignancies • Kussmaul´s disease (sialodochitis fibrinosa) • “signum mali ominis“ • acute postoperative sialadenitis 30% mortality !
Viralsialadenitides • sialotropic viruses • hematogennous spread during viremia • clinically evident sialadenitis • persistent infection reactivation • in saliva only (polio, lyssa, influenza, …) • Mi: interstitial non-purulent inflammation • dg.: serology
Parotitis epidemica • “mumps“ • paramyxovirus, childhood • air droplets upper airways + LN blood – viremia salivary glands • incubation period cca 18-21 days • clinically (up to ½ cases are inapparent !) • headache • uni- / bi-lateral swelling of parotis, event. submandibularis • symptoms for 10 days x infectious for 4-6 weeks ! • lifelong immunity
Parotitis epidemica • complications • in adults • 10-30 % orchitis (bilateral sterility?) • oophoritis • pancreatitis • meningoencephalitis • treatment: symptomatic • vaccination
Cytomegalovirussialadenitis • children • transplacental • per partum by cervical mucus • adults • immunosupression • generalized infection • saliva, transplantation, dialysis • + CMV hepatitis, myocarditis, polyradiculoneuritis • Mi: intranuclear inclusions in ductal epithelium “owl eye“
HIV in salivary glands • children (20 %), almost pathognomic for HIV ! • pathogenesis unclear • clinically • parotis swelling (in 60% bilateral), xerostomia • micro: • lymphoepithelial sialadenitis CD8+ (incl. LE islands) + lymphoid follicles • multiple lymphoepithelial cysts • diff. dg.: Sjögren´s syndrome
Chronicsialadenitides • chronic recurrent sialadenitides • chronic sclerosing sialadenitis • obstructive sialadenitis • pneumoparotitis • postactinic sialadenitis • specific sialadenitides • lymphoepithelial sialadenitis / Sjögren´s syndrome • sarcoidosis
Chronicrecurrentsialadenitides • from acute phase x de novo • parotis • changes of ducts • congenital, immunologic, postinfectious, obstruction • hyposialia + dyschylia + microliths • microscopy • lymphocytic inflammation + fibrosis + acinar atrophy • attack (7-10 days) + remission (months); trigger ???
Chronicrecurrentsialadenitides • children (Payen) • 3rd year peak 7th-10th year spontanneous regression • painful • adults • dg.: sialography – sialectasias of small ducts • treatment: rather conservative
Chronicsclerosingsialadenitis • Küttner´s “tumor“ (1896) • middle-aged and old patients • submandibular gland • clinically (diff. dg. malignancy) • bilateral x unilateral; focal x diffuse • firm painless swelling • microscopy • cellular fibrosis, lymphoplasmacellular inflammation, phlebitis • member of “IgG4-related disease“ !!! • treatment: corticosteroids, event. exstirpation
Obstructivesialadenitis • obstruction of ducts / papilla • sialolithiasis (most common) • tumors • injury • MSG – compression by dentures, smokers
Pneumoparotitis • increase of intraoral pressure • norm 3 mmHg; smt. up to 150 mmHg !!! • glassblowers, trumpeters • OC Stenon´s duct parotis constriction of facial muscles • event. subcutaneous emphysema • clinically • crepitations upon swollen parotis + air bubbles in saliva
Postactinicsialadenitis • complication of radiotherapy of HNSCCs • most vulnerable serous acini • hyposialia • 15 Gy – 50% of normal • 60 Gy – 10% of normal • risk factor for ascendent bacterial sialadenitis • MSG – xerostomia carries osteomyelitis • treatment: symptomatic, artificial saliva
Specificsialadenitides • tuberculosis • extremely rare • lymphogennous from oral cavity • --------------------------- • actinomycosis
Lymphoepithelialsialadenitis • = benign lymphoepithelial lesion (BLL), myoepithelial sialadenitis (MESA), Mikulicz´s disease (1892 ?) • Johann Freiherr von Mikulicz-Radecki (1850-1905) • x Mikulicz´s syndrome = swelling • + lymphoma, leukemia, … • parotis – 80-90% • clinically ± SS
Lymphoepithelialsialadenitis • microscopy • lymphoplasmacellular inflammation (CD4+) around small dilated ducts (MALT-like) proliferation of basal cells lymphoepithelial island = almost pathognomonic finding • variable acinar atrophy xerostomia • complications • extranodal marginal B-cell lymphoma (MALT lymphoma) – risk up to cca 20x higher (after7-10 years)!!! • carcinoma from lymphoepithelial islands • malignant lymphoepithelial lesion • Inuits • undifferentiated carcinoma
Sjögren´s syndrome • Henrik Samuel Conrad Sjögren (1899-1986) • = sicca syndrome, keratoconjunctivitis sicca • clinical syndrome: xerostomia ± xerophthalmia • middle-aged females (F : M …3-10 : 1) • variable involvement of all exocrine glands • autoimmune disease • Ab x ribonucleoprotein (RNP) • primary (40 %) • secondary (60 %) • + RA (10 % pts), SLE (30 % pts), sclerodermia, vasculitides
Sjögren´s syndrome • clinically in OC • difficult eating, swalloving, speaking • dry red mucosa • frequent infections, Candida • carries • risk of acute purulent parotitis • hyposialia • clinically in eyes • decrease production of tears, keratoconiunctivitis • sialography – sialectasias • laboratory findings • ABs anti-RO (SS-A) and anti-La (SS-B); RFs
Sjögren´s syndrome • microscopy • like lymphoepithelial sialadenitis • diagnostics: clinical findings + microscopy • labial MSG – so-called foci • treatment • artificial saliva, cholinesterase inhibitors • hygiene, fluorids and chlorhexidin locally • artificial tears • risk of MALT lymphoma !!! • SG damage is permanent !!!
Differential diagnosticsof xerostomia • organic causes • Sjögren´s syndrome • radiotherapy • HIV infection • sarcoidosis • amyloidosis • functional causes • dehydration • psychogennic (depression) • side effect of drugs
Sialolithiasis • middle-aged males (M : F … 2 : 1) • submandibular gland (85%) parotis (6-10%) • due to anatomy of Wharton´s duct • chemical composition of saliva • intraductal close to orifice (50%) intraductal intraparenchymatous • ethiology • changes in chemical composition of saliva due to infection and inflammation, Ca salts + nidus • clinically • salivary colic x asymptomatic • treatment – incision of duct orifice, exstirpation
Sialadenosis • non-inflammatory hypertrophy and hyperplasia of SG • disorder of innervation dyschylia • metabolic, endocrine, neurogennic disorders • malnutrition • alcoholism, liver cirrhosis • diabetes mellitus • dysfunction of thyroid gland • dysfunction of adrenal cortex • pregnancy, menopause • bulimia • drugs (antihypertensives, β-sympatomimetics, psycho-drugs)
Sialadenosis • bilateral painless swelling of parotis • recurrent x permanent • microscopy – 3x increased acini x NO inflammation • treatment ?
Cysts and fistulas • lymphoepithelial cyst • from epithelial inclusions in LN • middle-aged patients • unilateral, solitary • slowly growing painless swelling • x acute pain if secondary infection • microscopy • squamous / respiratory epithelium + lymphoid tissue in the wall
Cysts and fistulas • retention duct cysts • old males • well circumscribed painless swelling in parotis • blockage of the duct by detached epithelial cells • traumatic cysts / pseudocysts • mucoceles / ranulas • preauricular + cervicoaural fistulas
Necrotizingsialometaplasia • spontannous x iatrogennic microtraumata • middle-aged males, smokers • MSG of OC (hard palate), of nasal cavity, of larynx • ischemic necrosis (focal x diffuse) inflammation + reparation + squamous metaplasia of acini and ducts • clinically and microscopically mimics SCC !!! • painless ulcer about 2 cm with irregular margins • spontanneous healing within -2 months
Adenomatoid “hyperplasia“ • rare • middle-aged males • painless swelling of MSG on hard palate • clinically mimics tumor • microscopy • normal MSG, NO inflammation