Download
1 / 23
240 likes | 460 Views
Peripheral neuropathy: Prediction, prevention, and palliation February 9 2012 1640 - 1700. Beth Faiman, PhDc, MSN, APRN, BC, AOCN® Nurse Practitioner, Cleveland Clinic Taussig Cancer Institute PhD Candidate, Case Western Reserve University Cleveland, Ohio. Peripheral Neuropathy (PN).

E N D
Peripheral neuropathy: Prediction, prevention, and palliationFebruary 9 2012 1640 - 1700 Beth Faiman, PhDc, MSN, APRN, BC, AOCN®Nurse Practitioner, Cleveland Clinic Taussig Cancer Institute PhD Candidate, Case Western Reserve University Cleveland, Ohio
Peripheral Neuropathy (PN) • Damage to the peripheral nervous system caused by injury, inflammation, or degeneration of peripheral nerve fibers • Can affect QOL, compromise optimal treatments • Incidence of PN is increasing • More neurotoxic drugs have been developed • Patients are living longer, multiple treatment regimens • Multifactoral • Older age, chemotherapy dose/duration • Prior cisplatin or vinca alkaloids • Co-administration with other neurotoxic agents • Pre-existing conditions such as DM, ETOH, HIV positive, female gender, Vit B12 deficiency/B6 toxicity Tariman et al, 2008; Wickham, 2007; Thalomid® prescribing information, 2007; Velcade® prescribing information, 2009.
Peripheral Nervous System Peripheral nerve fiber Nervous system. On-line. Available: http://universe-review.ca/R10-16-ANS.htm , accessed 1/4/12.
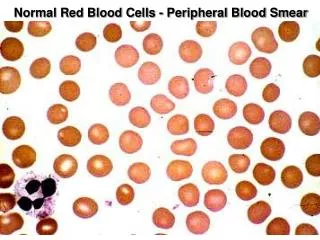
Peripheral Neuropathy (PN): General Concepts PN can lead to structural damage in the peripheral nerves of the central nervous system “Stocking-glove” distribution Sensory component of neuropathy has 2 primary types Small fiber: Pin-prick, pain and temperature Large fiber: Vibration and proprioception CIPN = chemotherapy-induced peripheral neuropathy. Armstrong et al, 2005. Ropper & Gorson, 1998
PN: Signs and Symptoms STOP • Symptoms: • Diminished or absent: • proprioception • vibratory sensation • touch sensation • sense of sharp/dull discrimination Tariman et al, 2008; Wickham, 2007.
Prediction: Chemotherapy Agents Associated with PN VAD= Vincristine, adriamycin, dexamethasone; DVD = Dexamethasone, vincristine, dexamethasone Cavaletti et al, 1992; LoMonaco et al, 1992; Mollman et al, 1988; Krarup-Hansen et al, 2007; Grothey, 2003; Quasthoff et al, 2002;de Gramont et al, 2000; Land et al, 2007; Pietrangeli et al, 2006; Dougherty et al, 2007; Verstappen et al, 2005; Chaudhry et al, 2003; Seidman et al, 2004; Winer et al, 2004.
Prediction: Chemotherapy Agents Associated with PN MM= Multiple Myeloma: Badros et al, 2007; Argyriou, Iconomou, et al, 2008; Jagannath et al, 2005; Gupta et al, 2006; Thomas et al, 2007; Buzdar, 2008; Argyriou, Koltzenburgh, et al, 2008; Chan et al, 1999; Thalomid® prescribing information, 2007.
Diagnosis of PN The diagnosis of PN is not straightforward PN “grading” can give us an idea as to severity Available grading scales have many limitations (wide variations in ones’ opinion) NCI Common Terminology Criteria for Adverse Events v4.0 (CT-CAE): Publish Date: May 28, 2009 PN = peripheral neuropathy.
Diagnostic Studies These are only a few of the available tests and procedures to diagnose PN Subjective and objective assessments are important to correctly diagnose PN Serum: • HIV, herpes, Vitamin B12 deficiency, B6 toxicity, CBC diff Radiology • X-ray, CT, MRI Neurodiagnostic studies • EMG • NCV • QST • Epidermal skin biopsy CT = computed tomography; MRI = magnetic resonance imaging; EMG = electromyography; NCV = nerve conduction velocity; QST = quantitative sensory test. Galer et al, 2000; Kovacs et al, 2006.
Assessment of PN • Diagnosis is often subjective • Patients will often volunteer change in sensation, gait or other signs of PN when asked • Evaluate sensory, motor and autonomic symptoms • Subjective assessment:Symptoms related to PN • Pain, numbness, burning, tingling, paresthesias, and autonomic signs • Objective assessment:Touch, vibration, gait and balance, proprioception, reflexes, muscle strength • Perception of sharp/dull are recommended as an adjunct to the subjective symptom assessment • Difficulty with fine motor skills: opening jars, buttoning Shy et al, 2003; Cavaletti et al, 2003; Dyck et al., 2000.
Assessment of PN Currently, no guidelines exist for the assessment or management of chemotherapy-induced peripheral neuropathy . • Monofilament (cutaneous touch) • Proprioception (rhomberg) • Test of motion and orientation • Sharp/Dull Perception • Pin Prick Test • Temperature sensation • Tuning fork, test tubes with water • Vibratory sense • 128 Hz tuning fork with the heel of the hand • Gait, muscle strength, reflexes Shy et al, 2003; Cavaletti et al, 2003; Dyck et al., 2000.
Patient Reported Symptoms FACT-GOG/neurotoxicity subscale: Most commonly studied in MM patients of all Total Neuropathy Scale (TNS) subjective and objective composite QLQ-CIPN 20 Almadrones instrument Neuropathy Impairment Scale GOG = Gynecologic Oncology Group; TNS = total neuropathy scale. Postma et al, 2005; Calhoun et al, 2003; Cella et al, 2003; Almadrones et al, 2004; Cavaletti et al, 1992.
FACT-GOG/ntx Neuropathy Assessment Tool Cella et al, 2003.
PN: Prevention and Management Strategies No prevention exists Regular monitoring at each treatment visit Neurotoxicity BEFORE EACH DOSE Treatment dose and schedule modifications- most effective Pharmacologic and nonpharmacologic interventions Patient education Dose reductions of bortezomib, thalidomide and other chemotherapy agents can prevent moderate to severe PN which impairs QOL Tariman et al, 2008; Wickham, 2007; Thalomid® prescribing information, 2007; Velcade® prescribing information, 2007.
Issues Surrounding Neurotoxicity Trials Few well-conducted trials in literature Sample sizes too small, underpowered Non-randomized, no placebo control Mix of chemotherapy agents allowed Mix of palliative and adjuvant setting Limited success in neurotoxicity prevention and treatment trials May be due to poor trial design, lack of nurse researchers Costs
Palliation: Pharmacologic Intervention Tricyclic antidepressants Anticonvulsants (gabapentin, lamotrigine) Vitamin E Glutamine Topical treatment IV = intravenous; Ca = calcium; Mg = magnesium. Cascinu et al, 2002; Armstrong et al, 2005.
Pharmacologic and Neuroprotectant Nortriptyline – Modest benefit, small study, lack of effectiveness Amitriptyline - Failed to improve sensory symptoms, but QOL improved Gabapentin, duloxetine and pregabalin - Studies failed to demonstrate benefit Lamotrigine – not effective Glutamine –Up-regulate nerve growth factor, decrease PN in a few previous trials Alpha-Lipoic- Acid Diabetic PN, may interfere w/ Bortezomib QOL = quality of life. Hammack et al, 2002; Kautio et al, 2008; Rao et al, 2007; Mitchell et al, 2006; Rao et al, 2008; Cascinu et al, 1995; Cascinu et al, 2002; Smyth et al, 1997; Wang et al, 2007.
Palliation: Non-Pharmacologic Acupuncture – limited data on PN No data in PN on Physical activity/exercise TENS (transcutaneous external nerve stimulation) Meditation/bio-feedback Pulsed infrared light therapy or anodyne therapy Armstrong et al, 2005; Arnall et al, 2006; Grothey, 2008.
Palliation: Practical Management of PN • Patient education • Notify clinician if signs and symptoms worsen • Home safety with decreased sensation in extremities • Caution patient on operating machinery • Family members to assess hot/cold if the patient is unable • Pharmaceuticals • Drug schedule and dose modifications of anti-myeloma therapy • Over-the-counter drugs • Vitamins/minerals/supplements – replace B vitamins, mag, ca++, glutamine • Amino acids (Glutamine, acetyl-L-carnitine, alpha lipoic acid) • Capsaicin, cocoa butter or emollients • Prescription drugs- No FDA-approved drug for PN • Unsure benefit of gabapentin, amitriptyline, sertraline, lidocaine patch Tariman et al, 2008; Wickham, 2007; Visovsky et al, 2007; Armstrong et al, 2005.
Case Study • Mrs. A is a 64 yo concert pianist diagnosed with stage II (ISS) IgG kappa MM • History DM, HTN • Starts induction therapy with bortezomib and dexamethasone • What should be taken into consideration prior to initiating therapy to prevent PN? • Occupation, co-morbidities • Patient education (self-reporting symptoms) • Patient completes Cycle 1 (uneventful) ISS = International Staging System; po = by mouth; ADL = activities of daily living. NCCN, 2009; Velcade® prescribing information, 2008.
Case Study • After Cycle 2 patient informs treatment RN that she has numbness without pain and continues to work (grade 1 PN) • Which is the best option to manage her PN? • Continue with Cycle 3 • Decrease dose • Discontinue therapy • Withhold therapy • After Cycle 4 she reports difficulty feeling the keys of her piano, but no pain (grade 2 PN) • Which is the best option to manage her PN? • Continue with Cycle 5 • Decrease bortezomib dose to 1.0 mg/m2 • Discontinue therapy • Withhold therapy until resolves Velcade® prescribing information, 2008; Argyriou, Iconomou, et al, 2008.
Additional Considerations for Patients at Risk for PN • Accurate baseline and ongoing assessment with a focused physical assessment of symptoms • Patient education • Safety!!! • Symptom reporting • Self-care strategies (exercise) • Discuss adjunct therapies with healthcare provider and monitor effectiveness • Referral for assistive devices to maintain ADL and prevent injuries from falls Wickham, 2007; Visovsky et al, 2007.
Key Takeaways: Patient Assessment There are no gold-standard, evidence-based recommendations for the assessment of PN Nurses are critical in early recognition and prompt intervention when symptoms of PN develop Baseline assessment of PN prior to the initiation of anti-MM therapy Identify individuals at risk for severe PN Educate if treatment must be given (Comorbid illness, prior treatments) Ongoing assessment of PN is recommended Hausheer et al, 2006; Wickham, 2007.