Download
1 / 32
320 likes | 334 Views
This chapter explains the main function of the respiratory system, which is to supply oxygen and eliminate carbon dioxide from the body. It explores the anatomy of the respiratory tract, including the nose, pharynx, larynx, trachea, bronchi, bronchioles, and alveoli. Additionally, it discusses the histology of the respiratory epithelium and the changes that occur in the airways as you go deeper into the bronchial tree.

E N D
The main function of the respiratory system is to supply oxygen to, & eliminate carbon dioxide from the body In order to accomplish this task, the respiratory system must work in conjunction with the cardiovascular system
“Respiration” refers to the overall exchange of gases between the atmosphere, blood & cells Respiration involves 3 processes • Pulmonary ventilation • Gas exchange (gas diffusion) • External respiration • Internal respiration • Gas transport
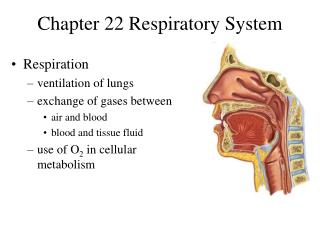
Anatomy Overview The respiratory tract includes: Nose (nasal cavity) Pharynx (nasopharynx, oropharynx, laryngopharynx) Larynx Trachea Bronchi (primary, secondary (lobar), tertiary (segmental) Bronchioles Terminal bronchioles Alveolar ducts Alveoli Nasal cavity Pharynx Larynx Trachea Bronchi Bronchioles Respiratory bronchioles Left Lung Right Lung Alveolar duct Alveoli
Histology Respiratory Epithelium = Pseudostratified Ciliated Columnar (PSCC)
Nose (nasal cavity) Air normally enters through external nares through nasal vestibule into nasal cavity. Functions of nasal cavity include: warming, moistening & filtering air; olfaction
Pharynx Air passes from nasal cavity into nasopharynx, past oropharynx & through laryngopharynx to larynx Nasopharynx lined with PSCC epithelium, but oro & laryngopharynx lined with stratified squamous epithelium
Larynx Air passageway made of 9 pieces of cartilage – (1) Thyroid cartilage, (1) Epiglottis, (1) Cricoid cartilage, (2) Arytenoid, (2) Corniculate, (2) Cuneiform A.K.A your “voicebox” because it contains the vocal cords
Thyroid cartilage – protects anterior & lateral walls of airway • Epiglottis – leaf-shaped cartilage that protects opening (“glottis”) of airway when swallowing • Cricoid cartilage – complete ring of cartilage; protects posterior wall of airway; attaches to trachea
Arytenoid, corniculate & cuneiform cartilages – attach to upper (false) vocal folds & lower (true) vocal cords
Trachea • Tough but flexible “windpipe”, anterior to esophagus • attached to cricoid cartilage (at about C6 vertebral level) & ends within mediastinum by branching into left & right primary bronchi (at T5 vertebral level) • End of trachea known as Carina Carina
Trachea • Lined with respiratory epithelium • “C”-shaped pieces of hyaline cartilage protecting airway while allowing for swallowing • Trachealis muscle (smooth muscle) runs across posterior wall of trachea connecting ends of tracheal cartilage
Bronchi • Trachea splits into a left & right primary bronchus which enters into the hilus (hilum) of each lung • Within the lung, the primary bronchi branch into secondary (lobar) bronchi (3 in right lung/2 in left lung) • Secondary bronchi then branch into 10 tertiary (segmental) bronchi • Tertiary bronchi then continue to branch into smaller & smaller bronchi & then into very narrow bronchioles Carina This branching patterns creates the “bronchial tree”
Changes In Airway As you go further down into the bronchial tree of each lung, changes in the airway occur: • increased number of airways (1 primary; 2 or 3 secondary; 10 tertiary bronchi; 6000 terminal bronchioles; millions of alveolar ducts) • decreased diameter of each airway • decreased amount of cartilage in the airways (no cartilage at all by terminal bronchioles) • increased amount of smooth muscle (relative to diameter) • lining epithelium changes from PSCC simple squamous epithelium (in alveoli)
Lungs Located within the thoracic cavity, surrounded by the double-layered pleural membrane – parietal pleura – lines cavity wall visceral pleura – covers the lungs
Apex – extends 1” above clavicle Hilum – at medial surface; where primary bronchus, pulmonary artery & veins enter/exit lung Superior lobe Superior lobe Horizontal fissure Oblique fissure Middle lobe Oblique fissure Cardiac notch Inferior lobe Inferior lobe Base – rests on diaphragm Lungs- Anatomical Features Right lung Left lung
Airways within Lungs • Each lung has a primarybronchus entering at the hilum • Each lobe of a lung has a secondary (a.k.a. lobar) bronchus • Lobes are functionally divided into bronchopulmonary segments & each segment has a tertiary (segmental) bronchus • Segments are functionally divided by elastic CT partitions into many lobules & each lobule receives a terminal bronchiole
Relationship of Airways & Pulmonary Vessels • As airways branch within lungs, they are accompanied by branches of the pulmonary artery (carrying de-oxygenated blood into the lungs), & branches of the pulmonary veins (carrying oxygenated blood out of the lungs) • As the alveolar ducts expand to form alveoli, pulmonary arterioles will branch to form a network of pulmonary capillaries, surrounding the alveoli
Alveoli • Alveoli are expanded chambers of epithelial tissue that are the exchange surfaces of the lungs • There are about 150 million alveoli in each lung • Multiple alveoli usually share a common alveolar duct, creating “alveolar sacs”
Alveoli There are three types of cells found within alveoli: • Alveolar Squamous epithelial (aka “type I”) cells – primary cells making up the wall of the alveoli • Septal (aka “type II”) cells – sectrete “surfactant” to reduce surface tension which prevents alveoli from sticking together & allows for easier gas exchange • Alveolar macrophages (aka “dust cells”) – phagocytic cells that remove dust, debris & pathogens
Gas “exchange” (external respiration) occurs across the Respiratory membrane – the fused membranes of the alveolar epithelium & the pulmonary capillary endothelium
Physiology of Respiration “Respiration” refers to the overall exchange of gases between the atmosphere, blood & cells Respiration involves 3 processes • Pulmonary ventilation • Gas exchange • External respiration • Internal respiration • Gas transport
Physiology of Respiration Pulmonary Ventilation – “exchange” (movement) of gases between the atmosphere & lungs; movement of gases occurs because of pressure differences between the atmosphere (atmospheric pressure (Po)) & lungs (intrapulmonic pressure (Pi)) Two phases of ventilation: • Inspiration • active process involving contraction of diaphragm & external intercostal muscles • Expiration • normally passive due to relaxation of above muscles • can be made active (forced expiration) due to contraction of abdominals & internal intercostal muscles
Lung Volumes & Capacities • Respiratory frequency (f) – number of ventilations (inspiration+expiration) per minute • Tidal volume (TV) - amount of air moved in or out of the lungs during a normal breath • Minute ventilation (VE=TV x f)- amount of air inhaled or exhaled in one minute
Lung Volumes & Capacities (cont.) • Inspiratory reserve volume (IRV) – amount of air that can be inhaled after a normal inspiration (above the resting TV) • Inspiratory capacity (IC = TV+IRV) – amount of air inhaled after a normal expiration • Expiratory reserve volume (ERV) – amount of air that can be exhaled after a normal expiration • Residual volume (RV) – amount of air remaining in lungs even after maximal expiration
Lung Volumes & Capacities (cont.) • Vital capacity (VC=TV+IRV+ERV) – maximum amount of air you can exhale, following a maximal inhalation • Total lung capacity (TLC=TV+IRV+ERV+RV) – maximum amount of air in your lungs, following a maximal inhalation
Gas Exchange (gas diffusion) • External respiration - the diffusion of O2 & CO2 between the alveoli & blood across the respiratory membrane • occurs because of pressure differences of each gas within alveolar air & pulmonary (deoxygenated) blood • results in creation of oxygenated blood
Gas Exchange • Internal respiration – the diffusion of O2 & CO2 between the blood & interstitial fluid across the endothelium of systemic capillaries • occurs because of pressure differences of each gas between systemic (oxygenated) blood & interstitial fluid • results in creation of deoxygenated blood
Gas Transport - O2 • During external respiration O2 diffuses across respiratory membrane into blood plasma • The majority of O2 (98.5%) then immediately diffuses into RBCs & binds (loosely) to the iron (Fe+3) in hemoglobin for transport • only 1.5% is transported freely dissolved within plasma
Gas Transport – CO2 • During internal respiration CO2 diffuses from interstitial fluid into plasma • Only 7% of CO2 remains in plasma for transport, the rest diffuses into RBCs • Within RBCs 23% binds to the globin proteins of hemoglobin (Hb) (“carbaminohemoglobin”) • Most (70%) of CO2 gets converted within RBCs to bicarbonate ions (HCO3-) – CO2 + H2O H2CO3 (carbonic acid) HCO3- + H+ HCO3- diffuses out to plasma (as Cl- diffuses in); the H+ attach to Hb to maintain normal plasma pH (so plasma does not become too acidic)
Control of Respiration Unconscious control of breathing occurs through the activity of the respiratory centers of the brain • Medulla oblongata – “Rhythmicity center” controls basic pattern of breathing; inhale 2 seconds, exhale 3 seconds • Pons – has 2 centers (apneustic & pneumotaxic centers) that can unconsciously modify the rate & depth of respiration Respiratory centers can be influenced by mechanoreceptors (i.e. stretch receptors in lungs) & chemoreceptors (sensitive to CO2 levels, arterial pH, & O2 levels) in the body, as well as by higher brain centers