Download
1 / 75
770 likes | 2.17k Views
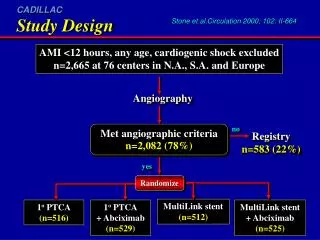
Care of The Post PTCA (Stent) Patient. Chris Kolyvas MD . Disclosures. I have nothing to disclose. Diagnostic Cardiac Catheterization vs. PTCA Number of Procedures Performed. Stents. Bare Metal Coil Slotted Tube Open/Closed Cell Covered Drug Eluting Sirolimus (Cypher)-Rapamycin-2003

E N D
Care of The Post PTCA (Stent) Patient Chris Kolyvas MD
Disclosures • I have nothing to disclose
Diagnostic Cardiac Catheterization vs. PTCA Number of Procedures Performed
Stents • Bare Metal • Coil • Slotted Tube • Open/Closed Cell • Covered • Drug Eluting • Sirolimus (Cypher)-Rapamycin-2003 • Everolimus (Endeavor)-2008 • Zotarolimus (Promus & Xience)-2008 • Paclitaxel (Taxus)-2004
Why Use Stents? • Nearly Eliminated Abrupt Vessel Closure • Significantly Reduced Restenosis • Reduced Urgent CABG
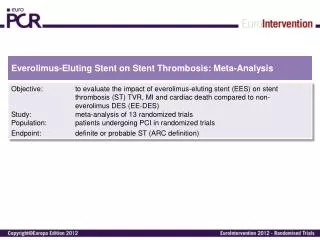
DES • Reduce Restenosis—TLR~4-5% a year • More Efficacious in Small Vessels, Long Lesions, Bifurcations, Diabetes • 4 Year Stent Thrombosis • ~1.2% DES—Metaanalysis Data • 0.6% BMS—Metaanalysis Data • Sirolimus vs Paclitaxel—Same • Everolimus (? Better)
AMI Left main Chronic renal failure Bifurcation Calcification Diabetes Diffuse disease Saphenous graft Multistenting Multivessel Ostium Unstable angina Thrombus Long lesions CTO DES Use “REAL WORLD”
DES vs BMS TAXUS IV SIRIUS Overall Restenosis (insegment) T=Paclitaxel S=Sirolimus T Control S Control
Initial Evaluation of PCI Patient in Office • Check for Vascular Complications • Hematoma • Retroperitoneal Bleed • Pseudoaneurysm
Vascular Complications • Insertion of vascular sheaths may produce groin or retroperitoneal hematomas • Groin hematoma presents with localized pain; lower extremity neurological symptoms are due to compression of the femoral nerve • Palpation of localized swelling or tenderness in the area, or loss of sensory or motor function is highly suggestive of a hematoma • Rates of major bleeding are decreasing (0.7% to 1.7%)
Retroperitoneal Hematoma • Low incidence (0.15% to 0.44%) • Should be suspected in patients with unexplained hypotension and/or marked decrease in Hct • Pts may experience flank, abdominal or back pain- • Note: absence of these symptoms does not exclude this condition
Retroperitoneal Hematoma • Diagnosis established by CT • Most treated conservatively; only 16% require surgery Kent, J Vasc Surg 1994;20:905-10
Pseudoaneurysm (PSA) • Communication between femoral artery and overlying fibromuscular tissue, resulting in a blood filled cavity • Incidence ranges between 0.5% to 6.3% • Groin tenderness, a palpable pulsatile mass and/or new bruit in groin should prompt examination by Doppler flow imaging • Most large PSA can be treated by US guided compression, US guided thrombin injection, or surgical repair • New technology to treat PSA is percutaneous PTFE covered stent graft
Acutestentthrombosis 24 hours incidence: 0.6% Short-term Prevention Sub-acutestent thrombosis Days to weeks incidence: <5% Late stent restenosis Up to 12 months incidence: 15% Major adverse cardiac events First year incidence: ~20% Long-term Prevention Other atherothrombotic events (all arterial beds) Life-long Secondary and Long-Term Prevention: Post-PCI
Stent Thrombosis is a Major Concern With BMS and DES • Acute 24 Hours • Subacute-1-30 Days • Late-30-365 Days • Very Late->365 Days
Timing of Late Stent Thrombosis Iakovou: JAMA 2005; 293: 2126-30
Presentation with DES Thrombosis Iakovou: JAMA 2005; 293: 2126-30
Late DES Thrombosis 2229 pts (SES:1062 ; PES 1167) % F/U through 9 mo Iakovou: JAMA 2005; 293: 2126-30
Predictors of Late Stent Thrombosis • Thienopyridine Discontinuation <6 months • Insulin Treated Diabetes • Lest Main Stenting • Smoking • Lesion Length >28mm • Multiple Stents • Moderate to Severe Lesion Calcification
Predictors of Late Stent Thrombosis (cont) • Reference Vessel Diameter <3 mm • Ostial lesions • Bifurcations • Low EF • Renal Failure • Suboptimal Stent Result • Platelet Nonresponsiveness
Reasons for Discontinuation • Cost • Lack of Education and F/U • Older Age • Bleeding/Bruising • Clopidogrel has Lower Risk of Bleeding than ASA
Methods to Prevent Premature Discontinuation • Discuss with Patient BEFORE Stenting • If Procedure Needed in Next 12 months, Consider BMS or Balloon PTCA • Educate Patients Post-Procedure • Instruct Patients to Contact their Physician Prior to Discontinue any Medication • Defer Elective Procedures if Possible
Oral Antiplatelet Agents Post PCI (Stenting) • Aspirin • Thienopyridines • Ticlopidine • Clopidogrel • Prasugrel
Ticlopidine • Initial Oral Thienopyridine • 1% Risk of Severe Neutropenia • Need CBC Monitoring • Rare TTP • Use in Patients Unable to Take Clopidogrel • Full Antiplatelet Action Takes Several Days
Clopidogrel • Most Commonly Used Thienopyridine in U.S. • Onset of Full Effect within Hours of a Loading Dose • Indicated in Patients After NSTEMI, U.A., STEMI
Prasugrel • Newest Thienopyridine • Triton TIMI-38 Trial—PCI • 13,680 Patients Randomized to Clopidogrel vs. Prasugrel • CV Death, MI, Stroke were Significantly Reduced in Prasugrel Group (9.9% vs. 12.1%) • Reduced Stent Thrombosis (2.4% vs. 1.1%) • Major & Minor Bleeding was Significantly Increased in Prasugrel Group • Not FDA Approved yet
Duration of Therapy Post PCI • Initially 2-4 weeks • PCI Cure Trial changed that • 31% Decreased Risk of CV Death, MI or Stroke with long term Clopidogrel • No Increase in Major Bleeding • Increase in Minor Bleeding • Credo Trial Found Similar Long Term Benefit Post—PCI • Based on these trials it is rec. ASA & Clopidogrel Post Stenting & PCI go to at least 1 year
Should Clopidogrel be used > 1 year in DES Patients? • Rationale is a small but increased risk of Late Stent Thrombosis in some DES Trials and Registries
Nonresponsiveness to ASA/Clopidogrel • 746 Patients • Complete platelet function Analysis • Nonresponsive to ASA = 11.5% • Clopidogrel Nonresponse = 6% • Both nonresponse= 6% • Responsive to Both = 0%
Noncardiac Surgery Post PCI • Defer Elective Surgery for 1 Year • If Surgery Needed After 3-6 months continue Low Dose Aspirin Periop. And Resume Clopidogrel Postop
Antithrombin Rx • If a Patient needs Warfarin (AF, valve etc.) and has a Stent Implanted, then ASA + Clopidogrel + Warfarin are needed • Little Data on this Topic • ? Increased Risk of Bleeding • Recent Registry Data Showed no Increased Death or Bleed 6 months Post Stent • Try and Keep INR Lower ~2.0 • Consider BMS • Each Clinical Situation Will Dictated How Aggressively to Anticoagulate
Acutestentthrombosis 24 hours incidence: 0.6% Short-term Prevention Sub-acutestent thrombosis Days to weeks incidence: <5% Late stent restenosis Up to 12 months incidence: 15% Major adverse cardiac events First year incidence: ~20% Long-term Prevention Other atherothrombotic events (all arterial beds) Life-long Secondary and Long-Term Prevention: Post-PCI
Risk Factors for Restenosis • Clinical Variables • Anatomic Variables • Procedural • Diabetes Mellitus Chronic Renal Failure (Dialysis) Unstable Onset Angina Recent Onset Angina • Saphenous Vein Graft (Aorto-osteal and body) Proximal left anterior descending artery Long Lesion Chronic Total Occlusions Restenotic Lesion Collateralized Distal Vessel Multiple Lesions ? Smaller Diameter Vessels • High Residual Stenosis ? Failure to Normalize Flow Reserve
Restenosis • Occurs over 1 to 8 months post PCI • Presenting symptoms include • exertional angina (25% to 85%) • unstable angina (11 to 41%) • MI (1 to 6%) Levine, Clin Cardiol. 1995;18:693-703
Evaluation for Restenosis • Prognosis for asymptomatic or “silent restenosis” is generally favorable • Routine periodic monitoring is not beneficial, indicated or recommended* • Hi risk pts should be followed: ↓ LVEF, multivessel CPD, PLAD lesion, • hx of sudden death, DM and hazardous occupation Ritchie, J. Am Coll Cardiol. 1995;25”521-47
Risk Factor Modification • Smoking Cessation • Cardiac Rehab & Exercise • Lipid Lowering • HTN Treatment • Weight Management
Smoking • Independent Risk Factor for CAD • 60% of Smokers Do Not Believe this • Incidence of MI is 3-6x increased • Patients with prior CAS have Increased risk of Death, Sudden Death, and Reinfarction • Pathogenesis— LDL + TG + HDL • Impaired Endothelial Function—Dose Related • Enhanced Prothrombotic State
Mediators • Nicotine—Sympathetic Neural Stimulation ( BP + HR + O2 Demand increases ischemia) • CO—binds to Hb and Increases Ischemia, Ventricular Dysfunction • Oxygen Free Radicals—Atherosclerosis development
Post-PCI—Smoking • Death—1.75x • Q wave MI—2x • 50% Decreased Reinfarction, Sudden Death & Mortality if Patients Quit
Cigarette Smoking Recommendations Goal: Complete Cessation and No Exposure to Environmental Tobacco Smoke • Ask about tobacco use status at every visit. • Advise every tobacco user to quit. • Assess the tobacco user’s willingness to quit. • Assist by counseling and developing a plan for quitting. • Arrange follow-up, referral to special programs, or pharmacotherapy (including nicotine replacement and bupropion. • Urge avoidance of exposure to environmental tobacco smoke at work and home.
Aberg, et al. 1983 0.67 (0.53-0.84) Herlitz, et al. 1995 0.99 (0.42-2.33) Johansson, et al. 1985 0.79 (0.46-1.37) Perkins, et al. 1985 3.87 (0.81-18.37) Sato, et al. 1992 0.10 (0.00-1.95) Sparrow, et al. 1978 0.76 (0.37-1.58) Vlietstra, et al. 1986 0.63 (0.51-0.78) Voors, et al. 1996 0.54 (0.29-1.01) Cigarette Smoking Cessation: Risk of Non-Fatal MI RR (95% Cl) Study 10 0.1 1.0 Ceased smoking Continued smoking • *Includes those with known coronary heart disease • CI=Confidence interval, RR=Relative risk • Critchley JA et al. JAMA. 2003;290:86-97.