Download
1 / 15
150 likes | 162 Views
Reconciling Disparate Results in Analyses of Stent Thrombosis in the use of Drug-Eluting Stents. “Per Protocol” Definitions of Stent Thrombosis. Early Stent Thrombosis ( ≤ 30 days) Thrombotic occlusion of the stented segment observed at the time of a clinically-driven angiographic restudy

E N D
Reconciling Disparate Results in Analyses of Stent Thrombosis in the use of Drug-Eluting Stents
“Per Protocol” Definitions of Stent Thrombosis Early Stent Thrombosis (≤ 30 days) • Thrombotic occlusion of the stented segment observed at the time of a clinically-driven angiographic restudy • Q-wave MI in territory of stented vessel • Any death not attributed to a non-cardiac cause Late Stent Thrombosis (>30 days) • MI attributable to the target vessel, with angiographic documentation of thrombus or total occlusion of the target site, and freedom from an interim revascularization of the target vessel CM Gibson 2006
ARC Definitions of Stent Thrombosis Definite/Confirmed • Acute coronary syndrome AND • Angiographic confirmation of stent thrombus or occlusion OR • Pathologic confirmation of acute stent thrombosis Probable • Unexplained death within 30 days • Target vessel MI without angiographic confirmation of stent thrombosis or other identified culprit lesion Possible • Unexplained death after 30 days • Note: Patients who have a TLR prior to stent thrombosis are included by this set of definitions, as opposed to the “Per Protocol” definition CM Gibson 2006
Potential Issues Arising From Different Definitions: Stent Thrombosis • Stent thrombosis may be angiographically confirmed in some analyses but not in other analyses. • If stent thrombosis is angiographically confirmed, the patient, by definition, survived until the time of angiography. It is therefore no surprise that angiographically confirmed stent thrombosis has a weak association if any with mortality. CM Gibson 2006
Potential Issues Arising from Different Definitions: Recurrent MI • If recurrent myocardial infarction is used in the definition, the definition of myocardial infarction should be provided. • Some analyses define MI as a Q wave MI. It should be realized that some patients with ST elevation will, and others will not, evolve a Q wave. Likewise, some patients with a non-STEMI elevation will go on to develop a Q wave. • More detailed data is needed to understand if the event was the result of recurrent ST elevation MI, or if the patient presented with a positive troponin without ST elevation. It is unlikely that restenosis presents with ST elevation MI, but it may present in some cases with a troponin elevation. • If ST elevation MI and troponin elevation are lumped together in the definition of recurrent MI this should be specified as they may carry quite different prognoses. CM Gibson 2006
Potential Issues Arising from Different Definitions: Mortality • It should also be specified if mortality was included in the definition, and if cardiac and non-cardiac mortality are being evaluated separately or together. • It is also often quite difficult to ascertain the true cause of death. The presence of a terminal illness such as cancer does not exclude the possibility that a patient may have sustained sudden death from stent thrombosis, particularly if the illness is associated with a prothrombotic state. CM Gibson 2006
Other Complications in DES Analysis • The analysis of stent thrombosis data can be complicated by other factors: • Both DES and BMS may be placed in the same patient. • DES from different manufacturers may be placed in the same patient. • A DES may be placed inside a BMS for restenosis. • Adjustments must be made for the concordance in the behavior of the stents. • Finally, thrombosis can occur outside of the stented segment. CM Gibson 2006
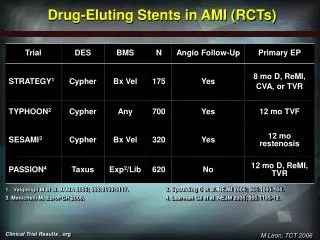
Randomized Trials vs Registry Data • Randomized trial data and registry data will provide different insights into the issue of stent thrombosis: • Randomized trial data does reduce the potential for confounding with respect to the procedural characteristics that led an operator to place either a bare metal stent or a drug eluting stent. • However, randomized trial data provides no guidance regarding clinical outcomes in more complex lesions and in patients with co-morbid conditions as these high risk lesions/patients are often excluded from randomized trials. CM Gibson 2006
Randomized Trials and Registry Data • While registry data does provide insight into “real world” practice patterns and outcomes, these data do not adjust for the fact that bare metal stents and drug eluting stents may be placed in different lesion/patient subsets. • For instance, in the DEScover Registry, a greater proportion of bare metal stents were placed in STEMI patients, and this patient population is at higher risk of mortality. CM Gibson 2006
Public Health Considerations • In placing these data in context from a public health perspective, it should be borne in mind that approximately 1 million stents are inserted each year. • It will be important to determine if the excess risk of stent thrombosis is confined to a limited period of time, or if the excess risk of stent thrombosis persists in each subsequent year after a drug eluting stent is placed. CM Gibson 2006
Lesion Revascularization and Stent Thrombosis over 20 years Speculative model comparing Lesion Revascularization vs Stent Thrombosis over 20 years • The model is based on a steady 0.5% rate of stent thrombosis each year • If a cohort of 1 million patients from 2006 is followed for 20 years with a stent thrombosis rate of 0.5% each year, this would yield over 95,000 stent thromboses within that cohort over a 20 year period CM Gibson 2006
Lesion Revascularization and Stent Thrombosis over 20 years • Even with the conservative estimate provided by the Cardiovascular Research Foundation group (1 thrombosis for 500 patient years of exposure), if a cohort of 1 million patients from 2006 is followed for 20 years, this would yield roughly 40,000 stent thromboses • At this conservative rate, the total number of stent thromboses over a 20 year period would be roughly 800,000. CM Gibson 2006
Thienopyridine Therapy • If there is in fact an excess of stent thromboses associated with DES use, prolonged thienopyridine therapy has been proposed as one solution to reduce the risk of thrombosis. • The potential benefit of prolonged thienopyridine therapy in reducing stent thrombosis, however, has not been evaluated in prospective randomized trials. • Prolonged thienopyridine therapy is not without risk and may be associated with a hazard of bleeding. • While there is a higher cost associated with DES vs BMS devices, the societal cost of treating millions of patients with prolonged thienopyridine therapy could be quite high as well. • The cost of prolonged thienopyridine therapy, the cost of stent thromboses and the excess cost of a DES vs a BMS must be weighed against the cost of repeat revascularization with BMS as well. CM Gibson 2006
Questions and Considerations • These data raise important questions regarding the adoption of new device technologies: • Should a new device (DES) replace a current device (BMS) if short term efficacy has been demonstrated in a surrogate endpoint (restenosis), but if long term safety data are not yet available? • How are we as a community to deal with the evaluation of catastrophic but infrequent adverse events? • Should the level of certainty surrounding safety be higher for a permanently implanted device than a drug which can be discontinued? • How many patient years of exposure in randomized trials is necessary before a permanently implanted device can be assumed to be safe? • What are the relative risks and benefits of drug eluting stents over aggressive medical therapy in the treatment of low risk patients with stable angina, given that the AVERT trial showed no benefit of percutaneous intervention in these patients (N Eng J Med 1999, 341: 70-76)? CM Gibson 2006
Conclusions • Future randomized trials of 8,000 to 30,000 patients have been proposed to evaluate the relative risks and benefits of DES vs BMS. • In parallel, efforts are also underway to develop standardized definitions of stent thrombosis to facilitate the comparison of trial data. CM Gibson 2006