Download
1 / 20
270 likes | 779 Views
Diagnosis and Treatment of Clavicle Fractures. Audience: Students in Health Care By Stephen Altano. Anatomical Review. The medical portion of the Clavicle attaches to the sternum The Lateral portion attaches to the acromion process of the scapula

E N D
Diagnosis and Treatment of Clavicle Fractures Audience: Students in Health Care By Stephen Altano
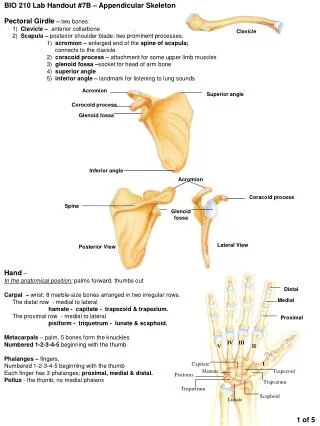
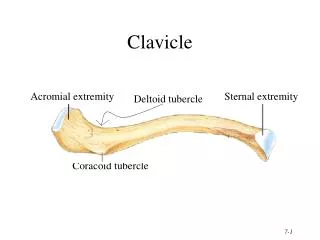
Anatomical Review • The medical portion of the Clavicle attaches to the sternum • The Lateral portion attaches to the acromion process of the scapula • Respectively comprising the acromioclavicular and sternoclavicular joints
Anatomy continued • Prevents anterior displacement of the scapula • Enables full range of motion of the arm • The Medial epiphysis is the last to ossify • Fuses at about 25 years old • The superior portion is not protected by muscle, making it vulnerable to injury
Mechanisms of Injury • The clavicle is most commonly fractured where the concave portion meets the convex • Mechanisms include; • Falling on tip of shoulder • Falling on outstretched arm • Direct impact • Clavicle fractures occur most commonly during Contact Sports • Is of the most common sports fracture • Football Fracture Video Example
Diagnosis Did you hear any sounds? I HERD A CRACK!
History • Athlete will describe a related mechanism • Complain of hearing a crack and crepitus • Have severe pain along the shaft of the clavicle • Can present neurological symptoms due to underlying neurovascular systems • Medical Emergency
Observation • Patient will be guarding • Holding arm with head tilted towards involved side • Obvious deformity will be present • Edema and ecchymosis
Motion, Strength, and Tests • All Motions will be limited • Patient will be apprehensive towards any movement • Strength testing is contraindicative • Percussion tests will be positive
Immediate Care • Ice • Sling and Swathe • Send to Emergency Room • X-Rays
Surgical Intervention • Most fractures are treated without surgery • Surgical Techniques • Plates and Screws • Pins
Surgical Intervention • Indications for Surgery • Neurovascular compromise • Excessive raised skin • Open fracture • Associated scapular fracture
Non-operative Treatment • Patient should be immobilized for up to six weeks • Can begin Range of motion exercises during immobilization period • All exercises should be pain free • Strength exercises should begin with isometrics and progress as motion is improved
Rehabilitation • Should be progressed based on symptoms and pain free activity • Therapeutic Modalities • Ice • Compression • Effleurage • Electric Stimulation • Ultrasound • Range of motion exercises • Passive • Active Assistive
Rehabilitation • Cardiovascular endurance • Stationary bike • Treadmill • Strength Exercises • Therabands • Manual resistance • Free weights • Plyometrics • Functional Activities • Sport or Job specific
Prognosis • Depends on type of fracture and patient • Typically 6 weeks for non-contact activities • Up to 12 weeks for contact sports • Important to Remember each case is unique
Return to Activity Criteria • Full range of motion • Strength is equal to uninvolved limb • No point tenderness over fracture site • Able to perform functional testing • Cleared by a physician • Psychologically ready
Sources • Ashwood N, Moonot P. Clavicle fractures. Trauma. 2009;11:123-132. • HouglamPA. Therapeutic Exercise For Musculoskeletal Injuries. 3rd ed. Champaign, IL: Duquesne University; 2010. • Pujalte GGA, Housner JA. Management of clavicle fractures. Current sports medicine reports. 2008;7:275