Download
1 / 69
710 likes | 929 Views
Epidemiology, Diagnosis Prevention and Management of Osteoporotic Fractures. Kenneth A. Egol, MD NYU-Hospital For Joint Diseases Created March 2004; Revised May 2006. Background. Osteoporosis -- a decreased bone density with normal bone mineralization WHO Definition (1994)

E N D
Epidemiology, Diagnosis Prevention and Management of Osteoporotic Fractures Kenneth A. Egol, MD NYU-Hospital For Joint Diseases Created March 2004; Revised May 2006
Background • Osteoporosis -- a decreased bone density with normal bone mineralization • WHO Definition (1994) • Bone Mineral Density ≥2.5 SD’s below the mean seen in young normal subjects • Incidence increases with age • 15% of white women age 50-59 • 70% of white women older than age 80
Background • Risk factors for osteoporosis • Female sex • European ancestry • Sedentary lifestyle • Multiple births • Excessive alcohol use
Background • Senile osteoporosis common • Some degree of osteopenia is found in virtually all healthy elderly patients • Treatable causes should be investigated • Nutritional deficiency • Malabsorption syndromes • Hyperparathyroidism • Cushings disease • Tumors
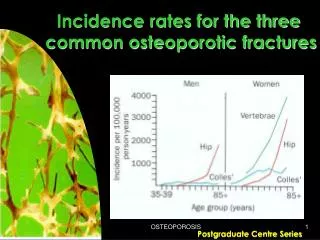
Background • The incidence of osteoporotic fractures is increasing • Estimated that half of all women and one-third of all men will sustain a fragility fracture during their lifetime • By 2050 --> 6.3 million hip fractures will occur globally • Enormous cost to society
Background • The most common fractures in the elderly osteoporotic patient include: • Hip Fractures • Femoral neck fractures • Intertrochanteric fractures • Subtrochanteric fractures • Ankle fractures • Proximal humerus fracture • Distal radius fractures • Vertebral compression fractures
Background • Fractures in the elderly osteoporotic patient represent a challenge to the orthopaedic surgeon • The goal of treatment is to restore the pre-injury level of function • Fracture can render an elderly patient unable to function independently --requiring institutionalized care
Background • Osteopenia complicates both fracture treatment and healing • Internal fixation compromised • Poor screw purchase • Increased risk of screw pull out • Augmentation with methylmethacrylate has been advocated • Increased risk of non-union • Bone augmentation (bone graft, substitutes) may be indicated
Pre-injury Status • Medical History • Cognitive History • Functional History • Ambulatory status • Community Ambulator • Household Ambulator • Non-Functional Ambulator • Non-Ambulator • Living arrangements
Pre-injury Status • Systemic disease • Pre-existing cardiac and pulmonary disease is common in the elderly • Diminishes patients ability to tolerate prolonged recumbency • Diabetes increases wound complications and infection • May delay fracture union
Pre-injury Status • American Society of Anesthesiologists (ASA) Classification • ASA I- normal healthy • ASA II- mild systemic disease • ASA III- Severe systemic disease, not incapacitating • ASA IV- severe incapacitating disease • ASA V- moribund patient
Pre-injury Status • Cognitive Status • Critical to outcome • Conditions may render patient unable to participate in rehabilitation • Alzheimer’s • CVA • Parkinson's • Senile dementia
Hip Fractures • General principles • With the aging of the American population the incidence of hip fractures is projected to increase from 250,000 in 1990 to 650,000 by 2040 • Cost approximately $8.7 billion annually • 20% higher incidence in urban areas • 15% lifetime risk for white females who live to age 80
Hip Fractures • Epidemiology • Incidence increases after age 50 • Female: Male ratio is 2:1 • Femoral neck and intertrochanteric fractures seen with equal frequency
Hip Fractures • Radiographic evaluation • Anterior-posterior view • Cross table lateral • Internal rotation view will help delineate fracture pattern
Hip Fractures • Radiographic evaluation • Occult hip fracture • Technetium bone scanning is a sensitive indicator, but may take 2-3 days to become positive • Magnetic resonance imaging has been shown to be as sensitive as bone scanning and can be reliably performed within 24 hours
Hip Fractures • Management • Prompt operative stabilization • Operative delay of > 24-48 hours increases one-year mortality rates • However, important to balance medical optimization and expeditious fixation • Early mobilization • Decrease incidence of decubiti, UTI, atelectasis/respiratory infections • DVT prophylaxis
Hip Fractures • Outcomes • Fracture related outcomes • Healing • Quality of reduction • Functional outcomes • Ambulatory ability • Mortality (25% at one year) • Return to pre-fracture activities of daily living
Hip Fractures • Femoral neck fractures • Intracapsular location • Vascular Supply • Medial and lateral circumflex vessels anastamose at the base of the neck • blood supply predominately from ascending arteries (90%) • Artery of ligamentum teres (10%)
Hip Fractures • Femoral neck fractures • Treatment • Non-displaced/ valgus impacted fractures • Non-operative 8-15% displacement rate • Operative with cannulated screws • Non-union 5% and osteonecrosis is approximately 8%
Hip Fractures • Femoral neck fractures • Displaced fractures should be treated operatively • Treatment: Open vs. Closed Reduction and Internal fixation • 30% non-union and 25%-30% osteonecrosis rate • Non-union requires reoperation 75% of the time while osteonecrosis leads to reoperation in 25% of cases
Hip Fractures • Femoral neck fractures • Treatment: Hemiarthroplasty • Unipolar Vs Bipolar • Can lead to acetabular erosion, dislocation, infection
Hip Fractures • Femoral neck fractures • Treatment • Displaced fractures can be treated non -operatively in certain situations • Demented, non-ambulatory patient • Mobilize early • Accept resulting non or malunion
Hip Fractures • Intertrochanteric fractures • Extracapsular (well vascularized) • Region distal to the neck between the trochanters • Calcar femorale • Posteromedial cortex • Important muscular insertions
Hip Fractures • Intertrochanteric fractures • Treatment • Usually treated surgically • Implant of choice is a hip compression screw that slides in a barrel attached to a sideplate • The implant allows for controlled impaction upon weightbearing
Hip Fractures • Intertrochanteric fractures • Treatment • Primary prosthetic replacement can be considered • For cases with significant comminution
Hip Fractures • Subtrochanteric Fractures • Begin at or below the level of the lesser trochanter • Typically higher energy injuries seen in younger patients • far less common in the elderly
Hip Fractures • Subtrochanteric Fractures • Treatment • Intramedullary nail (high rates of union) • Plates and screws
Ankle Fractures • Common injury in the elderly • Significant increase in the incidence and severity of ankle fractures over the last 20 years • Low energy injuries following twisting reflecting the relative strength of the ligaments compared to osteopenic bone
Ankle Fractures • Epidemiology • Finnish Study (Kannus et al) • Three-fold increase in the number of ankle fractures among patients older than 70 years between 1970 and 2000 • Increase in the more severe Lauge-Hansen SE-4 fracture • In the United States, ankle fractures have been reported to occur in as many as 8.3 per 1000 Medicare recipients • Figure that appears to be steadily rising.
Ankle Fractures • Presentation • Follows twisting of foot relative to lower tibia • Patients present unable to bear weight • Ecchymosis, deformity • Careful neurovascular exam must be performed
Ankle Fractures • Radiographic evaluation • Ankle trauma series includes: • AP • Lateral • Mortise • Examine entire length of the fibula
Ankle Fractures • Treatment • Isolated, non-displaced malleolar fracture without evidence of disruption of syndesmotic ligaments treated non-operatively with full weight bearing • My utilize walking cast or cast brace
Ankle Fractures • Treatment • Unstable fracture patterns with bimalleolar involvement, or unimalleolar fractures with talar displacement must be reduced • Treatment closed requires a long leg cast to control rotation • may be a burden to an elderly patient
Ankle Fractures • Treatment • Reductions that are unable to be attained closed require open reduction and internal fixation • The skin over the ankle is thin and prone to complication • Await resolution of edema to achieve a tension free closure
Ankle Fractures • Treatment • Fixation may be suboptimal due to osteopenia • May have to alter standard operative techniques • Cement Augmentation • Reports in literature mixed • Early studies showed no difference in operative vs non-op treatment -- with operative groups having higher complication rates • More recent studies show improved outcomes in operatively treated group • Goal is return to pre-injury functional status
Proximal Humerus • Background • Very common fracture seen in geriatric populations • 112/100,000 in men • 439/100,000 in women • Result of low energy trauma • Goal is to restore pain free range of shoulder motion
Proximal Humerus • Epidemiology • Incidence rises dramatically beyond the fifth decade in women • 71% of all proximal humerus fractures occur in patients older than 60 • Associated with • frail females • Poor neuromuscular control • Decreased bone mineral density
Proximal Humerus • Background • Articulates with the glenoid portion of the scapula to form the shoulder joint • Four parts • Combination of bony, muscular, capsular and ligamentous structures maintains shoulder stability • Status of the rotator cuff is key
Proximal Humerus • Radiographic evaluation • AP • Scapula Y • Axillary • CT scan can be helpful
Proximal Humerus • Treatment • Minimally displaced (one part fractures) usually stabilized by surrounding soft tissues • Non operative: 91% good to excellent results
Proximal Humerus • Treatment • Isolated lesser tuberosity fractures require operative fixation only if the fragment contains a large articular portion or limits internal rotation • Isolated greater tuberosity associated with longitudinal cuff tears and require ORIF
Proximal Humerus • Treatment • Displaced surgical neck fractures can be treated closed by reduction under anesthesia with X-ray guidance • Anatomic neck fractures are rare but have a high rate of osteonecrosis • If acceptable reduction is not attained open reduction should be undertaken
Proximal Humerus • Treatment • Closed treatment of 3 and 4 part fractures have yielded poor results • Failure of fixation is a problem in osteopenic bone • Locked plating versus prosthetic replacement
Proximal Humerus • Treatment • Regardless of treatment all require prolonged, supervised rehabilitation program • poor results are associated with rotator cuff tears, malunion, nonunion • Prosthetic replacement can be expected to result in relatively pain free shoulders • Functional recovery and ROM variable
Distal Radius • Background • Very common fracture in the elderly • Result from low energy injuries • Incidence increases with age, particularly in women • Associated with dementia, poor eyesight and a decrease in coordination
Distal Radius • Epidemiology • Increasing in incidence • Especially in women • Peak incidence in females 60-70 • Lifetime risk is 15% • Most frequent cause: fall on outstretched arm • Decreased bone mineral density is a factor
Distal Radius • Radiographic evaluation • PA • Lateral • Oblique • Contralateral wrist • Important to evaluate deformity, ulnar variance
Distal Radius • Treatment • Non-displaced fractures may be immobilized for 6-8 weeks • Metacarpal-phalangeal and interphalangeal joint motion must be started early
Distal Radius • Treatment • Displaced fractures should be reduced with restoration of radial length, inclination and tilt • Usually accomplished with longitudinal traction under hematoma block • If satisfactory reduction is obtained treatment in a long arm or short arm cast is undertaken • No statistical difference in method • Weekly radiographs are required