Download
1 / 1

E N D
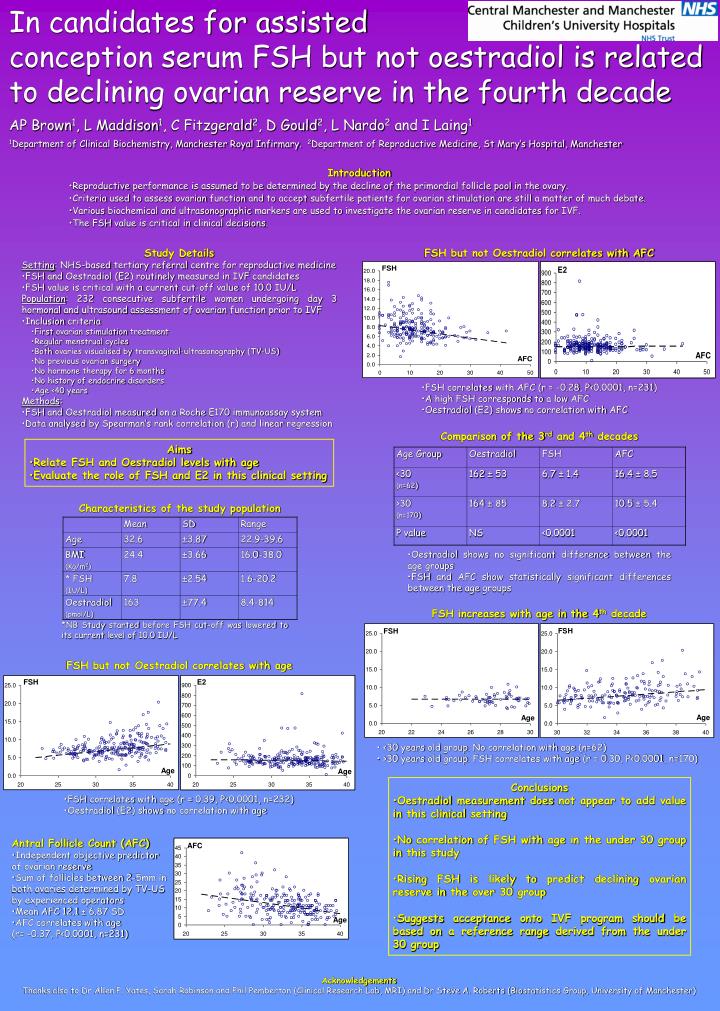
In candidates for assistedconception serum FSH but not oestradiol is related to declining ovarian reserve in the fourth decadeAP Brown1, L Maddison1, C Fitzgerald2, D Gould2, L Nardo2 and I Laing11Department of Clinical Biochemistry, Manchester Royal Infirmary. 2Department of Reproductive Medicine, St Mary’s Hospital, Manchester • Introduction • Reproductive performance is assumed to be determined by the decline of the primordial follicle pool in the ovary. • Criteria used to assess ovarian function and to accept subfertile patients for ovarian stimulation are still a matter of much debate. • Various biochemical and ultrasonographic markers are used to investigate the ovarian reserve in candidates for IVF. • The FSH value is critical in clinical decisions. FSH but not Oestradiol correlates with AFC • Study Details • Setting: NHS-based tertiary referral centre for reproductive medicine • FSH and Oestradiol (E2) routinely measured in IVF candidates • FSH value is critical with a current cut-off value of 10.0 IU/L • Population: 232 consecutive subfertile women undergoing day 3 hormonal and ultrasound assessment of ovarian function prior to IVF • Inclusion criteria • First ovarian stimulation treatment • Regular menstrual cycles • Both ovaries visualised by transvaginal-ultrasonography (TV-US) • No previous ovarian surgery • No hormone therapy for 6 months • No history of endocrine disorders • Age <40 years • Methods: • FSH and Oestradiol measured on a Roche E170 immunoassay system • Data analysed by Spearman’s rank correlation (r) and linear regression • FSH correlates with AFC (r = -0.28, P<0.0001, n=231) • A high FSH corresponds to a low AFC • Oestradiol (E2) shows no correlation with AFC Comparison of the 3rd and 4th decades • Aims • Relate FSH and Oestradiol levels with age • Evaluate the role of FSH and E2 in this clinical setting Characteristics of the study population • Oestradiol shows no significant difference between the age groups • FSH and AFC show statistically significant differences between the age groups FSH increases with age in the 4th decade *NB Study started before FSH cut-off was lowered to its current level of 10.0 IU/L FSH but not Oestradiol correlates with age • <30 years old group. No correlation with age (n=62) • >30 years old group. FSH correlates with age (r = 0.30, P<0.0001, n=170) • Conclusions • Oestradiol measurement does not appear to add value in this clinical setting • No correlation of FSH with age in the under 30 group in this study • Rising FSH is likely to predict declining ovarian reserve in the over 30 group • Suggests acceptance onto IVF program should be based on a reference range derived from the under 30 group • FSH correlates with age (r = 0.39, P<0.0001, n=232) • Oestradiol (E2) shows no correlation with age • Antral Follicle Count (AFC) • Independent objective predictor of ovarian reserve • Sum of follicles between 2-5mm in both ovaries determined by TV-US by experienced operators • Mean AFC 12.1 ± 6.87 SD • AFC correlates with age • (r= -0.37, P<0.0001, n=231) Acknowledgements Thanks also to Dr Allen P. Yates, Sarah Robinson and Phil Pemberton (Clinical Research Lab, MRI) and Dr Steve A. Roberts (Biostatistics Group, University of Manchester)


















