Download
1 / 20
200 likes | 299 Views
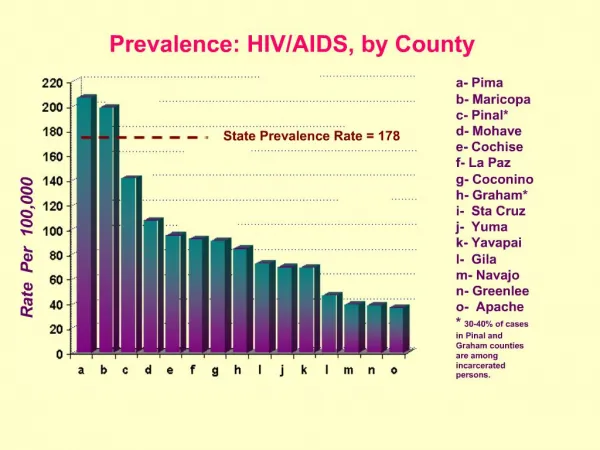
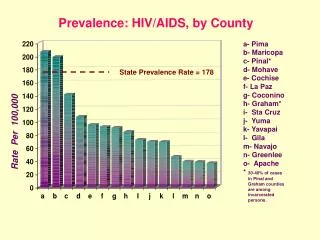
Prevalence of Obesity in HIV+ Population. Vickie Remoe Doherty AIDS Institute/Intern. HIV/AIDS prevalence US. Center for Disease Control (CDC) est. that annually there have been 40,000 new cases of HIV infection since the early 90s.

E N D
Prevalence of Obesity in HIV+ Population Vickie Remoe Doherty AIDS Institute/Intern
HIV/AIDS prevalence US • Center for Disease Control (CDC) est. that annually there have been 40,000 new cases of HIV infection since the early 90s. • In 2005, 38,096 cases of HIV/AIDS in adults, adolescents & children were diagnosed in 33 states w/ long-term name based HIV reporting • There are approx between 850,000-1,000,000 HIV-infected Americans
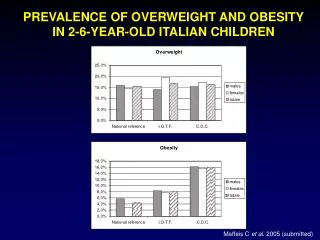
Obesity & Overweight In US • National Health and Nutrition Examination Survey (NHANES), using measured heights and weights, indicate that an estimated 66 percent of U.S. adults are either overweight or obese • Approx 127m adults=overweight, 60m obese & 9m extremely obese BMI>40 • Overweight defined as BMI >/= 25, Obese defined as BMI>/= 30
Nutrition & HIV Management • In the pre-HAART era (before 1996) malnutrition & wasting was common in HIV infection and was associated with diminished quality of life. Wasting was also a predictor of mortality and a sign of advanced HIV infection. • Nutritional management in the pre-HAART era consisted of managing wasting & malnutrition in HIV+ patients.
Nutrition & HIV Management • Since the availability of highly active anti-retroviral therapy (HAART) the incidence of malnutrition has reduced substantially, and US deaths due to HIV have decreased from 45,000(1995)-15,000(annually since 1997) • Several studies have identified obesity/weight gain as important complications in HIV/AIDS management in the HAART era (esp. for HIV+ women) • Obesity affects health, quality of life, and mental health
Nutrition & HIV Management • Overweight & obese persons w/ HIV infection are at an increased risk of developing metabolic and body composition abnormalities such as lipodystrophy, hyperlipidemia and insulin resistance associated with HIV infection and side effects from HAART medications.
Obesity Increases Risk of Other Diseases • Hypertension • Dyslipidemia (for example, high total cholesterol or high levels of triglycerides) • Type 2 diabetes • Coronary heart disease • Stroke • Gallbladder disease • Osteoarthritis • Sleep apnea and respiratory problems • Some cancers (endometrial, breast, and colon)
Obesity in HIV+ Population • Cross Sectional study of body shape & composition in urban cohort…characterizes body changes reported by women attending an urban US clinic • -163 women attending adult HIV outpatient clinic at J.Hopkins Baltimore/MD over 2mth Jul-Aug. Women >18yrs, HIV+…excluded pregnant, new to clinic, no documented VL/CD4 in past 3mths -BMI and weight/hip ratio calculated -based on patient results the following definitions were created lypodistrophy,weight loss, weight gain
Obesity in HIV pop • Results • -Data was available for 161/163 women. 42% of women who visited the clinic over 2mth period were enrolled in study. 89.4% Af.Am, Mode of trans reported sexual contact (54%) & IDU (40.4%)…w/77% of all subjects reporting history of cocaine, heroine & crack use. • 12/161 or 7.5% women reported body changes consistent w/ lipodystrophy, 27/161 or 16.4% reported weight loss and 85/161 or 52.8% described overall weight gain
Continued • Study suggests that obesity is an important issue for ethnic minority, in urban pops regardless of HIV status. • In accordance w/ other studies that suggest weight loss as an indicator of poor health. • In this study of HIV+ women, obesity and unhealthy, unintentional weight loss are greater than lipodystrophy in terms of prevalence. Most prevalent problem in cohort was weight gain and measured BMI confirming obesity • These results suggest that nutritional management may be most important for these populations as they are more at risk for obesity related illnesses such as heart disease and diabetes
Dietary Intake, Obesity in Urban Cohort • SMART/EST Women’s Project -466 HIV (receive stress management & nutrition education to test group vs. personalized counseling) - From Miami=191, NY & NJ= 186 Hypothesis-those who receive high intensity intervention (personalized w/ behavioral therapist) will have improved health & health behavior. Nutrition & Physical Activity Intervention focused on four components: identification of barriers to healthy eating, facilitator assisted self assessment of nutritional strengths and weaknesses, behavioral contracting to address participants highest priority nutrition/physical activity issues, monitoring behavioral progress adapting the behavioral contract as needed
Continued All measures collected by trained interviewers at baseline, 3mths (after completion of phase 1 CBSM+ interverntion),6mths(after completion of phase 2 health intervention),12mths(6 months after completion of full intervention) & 24mths (18 mths later). Used Rapid Eating Assessment and Activity Assessment for Patients (REAP) modified Subj in their 30s & 40s, women of color (Af.Am, Latina, Haitian =91%). Most (88.4%) reported incomes of $10,000 or less per year. -Many of the participants were overweight/obese- -Mean BMI 28.1
What participants reported eating At the beginning of the study 43% of the participants reported drinking more than 16ounces of sweetened beverages a day 30.4% ate sweets more than twice a day 34% ate fried foods more than twice a day Participants in Miami & NY/NJ differed in REAP-S in 10/13 indv questions Miami participants ate less frequently in restaurants, ate more fruit, fewer full fat chips and added less fat at the table NY/NJ participants reported more whole grains, vegetables, milk products and lower consumption of high fat cold cuts, sweets & sweetened beverages NY/NJ participants had more central obesity as showed with higher waist to hip ratio
Which intervention worked? • No differences in improvement b/n the two geographic sites- however those who received the initial high intensity intervention initially improved more than those with who received low intensity treatment. But at 18 months post intervention there were no differences between those in the high intervention group versus those in low intervention. • Benefits of high intensity nutrition intervention without reinforcement eventually taper off over time. • All groups improved their food group choices by decreasing fats and sugars but did not increase vegetables, fruits or whole grains (most likely due to price, lack of familiarity, taste, and availability in low income areas) • Results suggest those who provide nutritional education/counseling should be aware of barriers to accessing healthy foods
Obesity in HIV+ populations Cross sectional DEXA Substudy in the Women’s Interagency HIV study (WIHS) -271 women in Bronx/Manhattan -53 women in San Francisco • Participants also asked about #hrs spent exercising, type of exercise, smoking habits, current & nadir CD4, viral load, co-infection w/ hep C or B and social and medical history • Women were then divided into HIV positive & negative. The positive group was further divided into (no ART=70),(HAART/PI n=48), HAART/noPI=53. 12 HIV+ women were on ART that did not meet HAART criteria and were excluded from analyses on differences in HIV positive women • 88 (HIV negative), 183 HIV+were enrolled and were matched in terms of racial distribution…majority of women identified as ethnic minorities and there was no significant difference (HIV+/-) for exercise level, education level, # women trading sex for money or # male or female partners
Results from DEXA WIHS Substudy Majority in both groups overweight/obese -HIV- Overweight & obese(75% or 66/88 ) HIV+ overweight & obese (68% or 125/183) Factors assoc w/ total and regional fat in HIV+ women exercise (>6hrs/wk) was the only factor assoc w/ lower total, trunk & leg fat. Af. Am had sig. more leg fat than other ethnic groups -Study provides evidence of sig lower levels of leg fat in HIV infected women on HAART when compared with both HIV- women and HIV+ women currently using ART Suggests that medication may not be responsible for patient weight gain and obesity; rather that nutritional management should be used to help patients decrease food intake and develop healthier eating habits
Another study in HIV+ youth in US Extracted from the Reaching for Excellence in Adolescent Care & Health Study -cross-sectional study during one visit Jan-Oct 2000 -264 HIV+ youth vs. 127 HIV- aged 13-23, at 14 clinic sites in US -(75% women, 67% Af-Am 20.5% Hispanic) -calculated BMI, dietary intake, diet quality, CD4/VL & demographic info, socioeconomic, health & health behavior RESULTS -Avg BMI was 28, 51% of participants were obese/overweight. 6 mth avg weight gain 1.5. Obese participants gained more weight than non-obese participants. 49% of HIV infected were obese vs. 54% of HIV-prevalence of obesity decreased with lower cd4 (more significant for obese HIV+ female) -participants from S&NE 4x more likely to be obese than Chicago or LA. Race/ethnicity & economic not sig predictors of obesity -For Healthy Eating Index (HEI) that measured food intake, 68% had diet that needed improvement, 31% had poor diets. HIV+ had poorer diet than uninfected
Does diet & Exercise work for hiv+ obese? • 12 week prospective study longitudinal pilot study weight reduction intervention with diet management & aerobic/resistance • Women >18yrs old, obese w/BMI>30, on art and clinically stable @ St Luke’s, NY • Subjects received individual counseling at the beginning and thru out trial period by participating in weekly nutrition education classes • Subj exercised 90 mins w/ trainer 3x week. Asked to completed food diaries • Of 45 women screened, 39 were eligible and 18 completed the intervention • The avg loss after 12 weeks was 6.7kg(2.2lbs/kg) or 7.3% of initial weight -This study suggests that caloric restriction, nutritional education and exercise are just as effective for weight loss in hiv+ women
Conclusions • Obesity is prevalent in HIV+ pops esp (urban, women of color, disadvantaged) • Some reasons for obesity high caloric intake, poor quality diet w/ sugar & high fat content, not enough exercise, lack of availability/access to better quality foods • Being on medication alone does not explain obesity/weight gain in hiv+ pops though some meds cause abnormal accumulation of fat in body
Conclusions continued • Nutritional education, exercise, lower caloric intake can help reduce weight gain & obesity in HIV+ patients • Different interventions: group education/ personalized nutritional intervention also helpful • Obesity also prevalent in HIV+ youth • To improve short and long term health outcomes we must improve provide optimum nutritional education & services that can help change eating habits, decrease obesity & weight gain and improve overall quality of life