Download
1 / 78
1.04k likes | 2.55k Views
Urinary Bladder Cancer. John Crew, M.D., PGY-2 Radiation Oncology Brown Cancer Center, University of Louisville. Outline. Overview Anatomy Etiology/Epidemiology Risk Factors Pathology Clinical Presentation, Diagnosis, Work-up Staging Literature Review Conclusions Questions. Anatomy.

E N D
Urinary Bladder Cancer John Crew, M.D., PGY-2 Radiation Oncology Brown Cancer Center, University of Louisville
Outline • Overview • Anatomy • Etiology/Epidemiology • Risk Factors • Pathology • Clinical Presentation, Diagnosis, Work-up • Staging • Literature Review • Conclusions • Questions
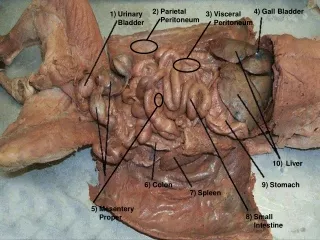
Anatomy http://academic.kellogg.edu
Etiology/Epidemiology • 2009 • 70,980 new cases of bladder cancer • 14,330 deaths from bladder cancer • Median age: 73 y • M:F – 3:1 • Caucasian predominance • 90% > Age 55
Incidence http://www.cdc.gov
Death Rates http://seer.cancer.gov/
Clinical Presentation • Painless Hematuria • Intermittent, gross, painless • ~10-20% with gross hematuria/~2-5% with microscopic hematuria diagnosed with bladder cancer • Pain • Flank • Suprapubic • Hypogastric/Perineal pain • Abdominal/RUQ • Distant sites • Voiding • Functional changes/obstruction • Irritation • Constitutional • Fatigue, weight loss, anorexia, renal failure, FTT
Lymph Nodes at Risk • Primary Drainage • Hypogastric • Obturator • Iliac (External, Internal, NOS) • Perivesical Pelvic, NOS • Sacral (lateral, sacral promontory (Gerota’s) • Presacral • Secondary Drainage • Common Iliac • Para-aortic
Metastatic Sites • Lung • Bone • Peritoneum
Physical Exam • Complete • Abnormal findings: • Solid pelvic mass • Induration of prostate • Inguinal adenopathy • Nodularity at periumbilical • Hepatic enlargement
Urologic evaluation • U/A; Urinary Cytology • Evaluation of upper urinary tract • CT abd/pel • EUA/Cystourethroscopy • Detailed description of size, number, appearance, location, and growth pattern • Biopsy/Transurethral resection • Include suspicious lesion, any sites of previous bladder tumor, grossly normal epithelium, prostatic urethra
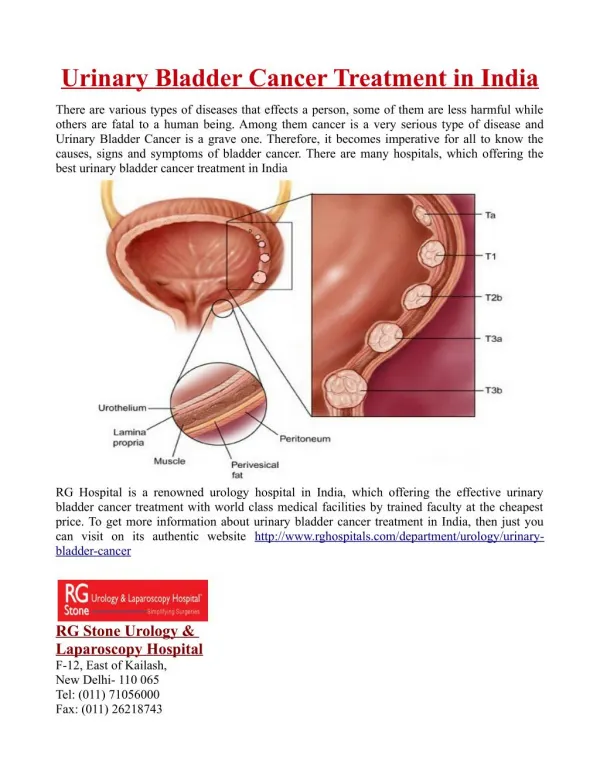
http://www.emoryhealthcare.org/urology/oncology/bladder-cancer/bladder-cancer-grading-staging.htmlhttp://www.emoryhealthcare.org/urology/oncology/bladder-cancer/bladder-cancer-grading-staging.html
T Staging TURBT Surgeon - Pathologic Organ Conservation – Clinical (TURBT: can see understaging)
Histopathologic Type • Urothelial Carcinoma (Transitional Cell) • In Situ • Papillary, Flat, Squamous Differentiation, Glandular Differentiation, Squamous/Glandular Differentiation • Variants: Micropapillary and Nested subtypes • Squamous Cell Carcinoma • Adenocarcinoma • Undifferentiated Carcinoma
Carcinoma in situ http://www.webpathology.com http://www.realwire.com
Urothelial, High Grade Johns Hopkins Pathology http://path.upmc.edu/cases/case15/images/gross1.jpg
http://www.rtog.org/members/protocols/0926/0926.pdf Slide adapted from: Shipley, Zeitman. An update of bladder conservation by tri-modality therapy in muscle-invasive cancer. ASTRO Refresher, 2009.
Treatment Modalities • Local • Surgery • Radical Cystectomy, Lymphadenectomy and Urinary Diversion • Radiation Therapy • Systemic • Chemotherapy • Adjuvant and Neoadjuvant
Radical Cystectomy Technique • Males • Bladder • Prostate • Seminal Vesicles • Females • Bladder • TAH/BSO • Anterior Vagina • Urethra http://www.memhc.org
Urinary Diversion • Incontinent cutaneous • Cutaneous continent • Requires self catheterization of reservoir • Orthotopic neobladder • Segment of bowel attached to urethra • Patients able to voluntarily void
Fig 2. (A) Recurrence-free survival and (B) overall survival in 1,054 patients after radical cystectomy stratified by pathologic stage and lymph node status Stein, J. P. et al. J Clin Oncol; 19:666-675 2001
Stein et al: Organ confined, lymph node negative tumors • 56% pts • 5/10 yr RFS: 82%/85% • No difference in survival • Tis, Ta, T1, T2a, T2b • Supports definitive surgical management for this group
Extravesical, Lymph Node – Negative Tumors • 20% of patients • No survival difference between pT3 and pT4 • 5y/10y RFS: 58%/55% • LN involvement: 45% • Assoc. with higher recurrence, decreased survival
Stein et al.: Lymph Node + • ~25% with path positive nodes • Risk increases with T stage • 33% alive at 5 yrs • Survival predicted by extent of dissection • # nodes sampled • Node Density http://training.seer.cancer.gov
Pelvic Node Dissection • Standard Template • Distal Common Iliac, Obturator, Hypogastric, External Iliac • Extended template • Standard + presacral, common iliac nodes to aortic bifurcation, more proximal to origin of inferior mesenteric • Data suggesting standard template inadequate • 290 patients, mapping studyusing extended template • 28% cases with positive nodes, 25% had nodes restricted to standard template, 25% had all nodes outside standard template
LN staging (2010) • Nx: Nodes not assessed • N1: Single Node in the true pelvis (hypogastric, obturator, external iliac, presacral) • N2: Multiple regional nodes in true pelvis • N3: Common iliac nodes
Surgical Morbidity • General • MI, PE, DVT • Impotence (100%) • Urination • Incontinence (15-40%), Enuresis (30%), Hypercontinence (15%, women), • Sexual Dysfunction • Cavernous nerve injury
Nerve-sparing Surgical Technique http://urology.jhu.edu
Nerve-sparing Surgical Technique • Concern for positive margins • LR ~3-5% • Comparable to patients managed without nerve sparing • Erectile Function • 31-50% patients within one to two years • Most requiring PDE-5 inhibitor • Prostate sparing surgery • Highly selected patients with good outcome • Concern for oncologic efficacy
Recurrence Following Surgery • Correlates well with stage and subgroup • USC experience (Stein et al.) • 30% patients fail locally/distant • Median time to rec. (Any/Local/Distant): 12m/18m/12m • Pelvic recurrence: 7% • 6% with OC tumors • 13% with EV tumors • Nearly all pts succumb • Distant Recurrence: • 13% with OC/LN- • 32% with EV/LN- • 52% with LN+ • 86% recur within 3 years post-op • Need for diligent surveillance
Neoadjuvant Chemotherapy • High risk for distant metastasis in muscle invasive disease • Advantages: • Theoretical benefit in eliminating micrometastases prior to surgery • Can evaluate responsiveness of a lesion • Downstaging • Disadvantages • Discordance between clinical and pathologic staging • Exam suggests CR, but path shows PR • Delay of local therapy
MRC/EORTC • 491 pts, high grade T2-T4a, N0-Nx, M0 urothelial • 3 cycles of cisplatin, methotrexate, vinblastine (MCV) or no chemo followed by RT or cystectomy (institution choice) • pCR (CMV): 33% • Absolute OS improvement of 5.5% for chemo (NS) • 7 yr update (NS)
INT 0080 • 317 pts, T2-4a N0M0 urothelial • Methotrexate, vinblastine, doxorubicin, cisplatin (MVAC) x 3 + cystectomy v. cystectomy alone • F/u 8.7 yrs • pCR 38% v. 15% • MS: 77 mo. v. 46 mo. (p = 0.06) • 5 yr OS: 57% v. 43% (p = 0.06) • 30% with ≥ grade 3 hematologic/GI effects, no treatment related deaths
Retrospective review using SWOG database • Surgical factors have prognostic significance? • Found: optimal cystectomy and lymph node dissection (negative margins and at least 10 node) associated with survival (>80% at 5 yrs) • INT 0080 not designed for this analysis, subject to confounders
Italian Bladder Tumor Study Group • 171 pts, T2-T4, N0, M0 urothelial • Methotrexate, vinblastine, epirubicin, cisplatin (MVEC) + cystectomy v. cystectomy alone • Not published • NS for DFS, OS at 33 mo f/u in prelim report • Clinical staging accurate in 42% • 23% overstaged • 33% understaged
Nordic 1 • 325 pts, high grade T1, or stages T2-T4a, Nx, M0 urothelial • 2 cycles cisplatin/doxorubicin + RT and Cystectomy • 5 yr f/u • OS: 59% v. 51% • Cancer specific survival (CSS): 64% v. 54% • Subset analysis (T3/4): • 15% OS, 20% CSS benefit with chemo
Nordic 2 • Prospectively defined subgroups • 317 pts, T2-T4aNxM0 urothelial • Cisplatin, Methotrexate +cystectomy v. cystectomy alone • 5 yr OS: 53% v. 46% in favor of neoadjuvant (SS)
Metaanalysis Platinum based combination chemo: 13% improvement in relative risk of death