Download
1 / 45
450 likes | 560 Views
Echocardiography & Endocarditis . Echo Imaging Conference 1/20/10 Ethan Ellis, MD. Overview. Background Diagnosis ACC/AHA indications for Echo TTE versus TEE Diagnostic Echo criteria Echocardiographic estimation of outcome Intracardiac complications of endocarditis

E N D
Echocardiography & Endocarditis Echo Imaging Conference 1/20/10 Ethan Ellis, MD
Overview • Background • Diagnosis • ACC/AHA indications for Echo • TTE versus TEE • Diagnostic Echo criteria • Echocardiographic estimation of outcome • Intracardiac complications of endocarditis • Surgical indications by Echocardiography
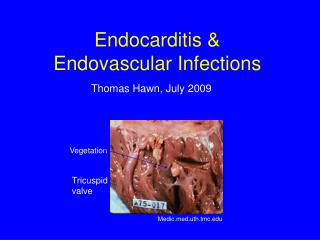
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits • Diagnosis: modified Duke criteria
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits • Diagnosis: modified Duke criteria • No noninvasive technique can definitively diagnose • Echocardiography has high sensitivity for IE and intracardiac abscess • Mandatory in the diagnosis and treatment of IE • ACC/AHA 2006 guidelines on valvular heart disease include recommendations for Echo use in native and prosthetic valve IE
Goals of Echo in Possible IE • Identify, localize, and characterize masses consistent with vegetations • Identify new valvular regurgitation • Examine prosthetic valve stability • Apply criteria to judge prognosis once vegetation identified
Accuracy of TTE • Meta analysis 1984: 641 pts* • Mean sensitivity of 79% for detecting veg’s • More recently, decreased sensitivity despite tech improvements • 7 studies, 1989-1994, Mean sensitivity of 62% 4-11 • ? d/t more rigorous case selection or d/t decreased TTE scrutiny now with TEE • Limitations • Underestimates size and complexity of large veg’s • May fail to detect small veg’s (< 3 mm) *O'Brien, JT, Geiser, EA. Infective endocarditis and echocardiography. Am Heart J 1984; 108:386
Accuracy of TEE • More invasive and expensive than TTE • High sensitivity in detecting and defining valve vegetations • Same 7 studies from 1989-1994, sensitivity 92% (compared to 62%)4-11 • 5 studies w/ similar results for sensitivity also revealed high specificity for TEE and TTE (93% vs 46% sensitivity, 96% vs 95% specificity) 4,8,10-12 • ACC/AHA guidelines, main role of TEE is: • Nondiagnostic TTE • Prosthetic valve endocarditis • Assessment of complications
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material • Motion: choatic and orbiting, independent of valve motion • Prolapse into upstream chamber (i.e. MV mass into LA in systole)
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material • Motion: choatic and orbiting, independent of valve motion • Prolapse into upstream chamber (i.e. MV mass into LA in systole) • Shape: lobulated, amorphous • Accompanying abnormalities: • abscess, pseudoaneurysm, fistula, prosthetic dehiscence, paravalvular leak, new regurgitant lesion
Diagnostic Echo criteria Characteristics of mass unlikely to be vegetation: • Texture: reflectance of calcium or pericardium (white) • Location: outflow tract attachment, downstream surface of valve • Shape: stringy or hair-like strands with narrow attachment • Lack of accompanying turbulent flow or regurgitation
False Positives • Most common on TEE • Lambl’s excrescences • Strands on sewing rings of prosthetics • Free suture • Redundant chordae, false tendons in LV • Chiari’s remnant in RA • Chordal insertion into normal MV • All of above tend to be highly reflective with echodensity similar to pericardium or aortic root. Dense, fibrotic, non-vibratory nature
False Negatives • TTE>TEE • High sensitivity of TEE (92-94%) • Cannot definitively rule out endocarditis • Low likelihood of IE if negative TEE in intermediate probability patient • In patients at high risk for IE (prosthetic valve, unexplained bacteremia), repeat examination reasonable
Echo Estimation of Outcome • TTE: • 1991 Retrospective study. 204 pts with clinical criteria for IE.* • Clinical complications (drug failure, new CHF, embolization, surgery, death) compared to vegetation characteristics • Overall complication incidence 55% • Rates similar between native and prosthetic valves as well as between MV, TV, and AV • Size of vegetation most powerful predictor of complication • 10% if 6 mm vegetation, 50% if 11mm vegetation, almost 100% if > 16 mm • Complications more frequent with higher grades of mobility and lesion extent • Vegetation consistency did not predict complications (except for calcified lesions which had no associated complications) *Sanfilippo, AJ, Picard, MH, Newell, JB, et al. Echocardiographic assessment of patients with infectious endocarditis: Prediction of risk for complications. J Am Coll Cardiol 1991; 18:1191.
Echo Estimation of Outcome • TEE: • Observations on TTE not directly applicable to TEE since given vegetation likely to appear larger on TEE • 105 pts with IE, 1989*: • vegetation > 10 mm = increased incidence of embolization (47% v 19%, p<0.01) • Association particularly strong for MV endocarditis • Vegetation size and location did not predict other rates of complications (CHF, death) • 178 pts with IE, 2002+: • Vegetation mobility confers additional risk beyond vegetation size • Embolic incidence higher with vegetation > 15 mm (70% vs 27%) and when vegetation moderately or severely mobile (62% vs 20% compared to low mobility) • Embolic rate 83% with large and severely mobile vegetations • Observational studies suggest risk of embolism declines after institution of antibiotic therapy • Echo predictors still apply after initiation of antibiotics • Greater vegetation size and mobility still predicted late embolic events • Increase in vegetation size after antibiotic start also predicted prolonged healing phase and a higher embolic risk *Mugge, A, Daniel, WG, Frank, G, Lichtlen, PR. Echocardiography in infective endocarditis: reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J Am Coll Cardiol 1989; 14:631. +Di Salvo, G, Habib, G, Pergola, V, et al. Echocardiography predicts embolic events in infective endocarditis. J Am Coll Cardiol 2001; 37:1069.
Intracardiac Complications • Valvular regurgitation • Secondary infection of other valves • Leaflet perforation
Intracardiac Complications • Valvular regurgitation • Secondary infection of other valves • Leaflet perforation • Perivalvular abscess or fistula • Early invasion cellulitis (echodense thickening of perivalvular tissue) Necrosis and inflammation abscess cavity • Abscess most likely with staph aureus • Risk of fistula formation • Abscess formation increase in morbidity and mortality • TEE >TTE: 118 pts with IE, 1991, 44 with abscess at surgery/autopsy. 87% vs 28% sensitivity* • TEE still imperfect. Additional series 2007 showed TEE detecting only 48% of abscesses (21 of 44 pts)+ *Daniel, WG, Mugge, A, Martin, RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991; 324:795. +Hill, EE, Herijgers, P, Claus, P, et al. Abscess in infective endocarditis: the value of transesophageal echocardiography and outcome: a 5-year study. Am Heart J 2007; 154:923.
Right Sided Endocarditis • Tricuspid valve vegetations most common in IV drug users • Most caused by staph aureus • Infrequently, R sided endocarditis due to involvement of PV • Often diagnosed only by TEE • most literature limited to single case reports • Most reports of R sided endocarditis have used TTE • In 48 IVDU pts with suspected IE, 22 with vegetations+ • TTE and TEE equally sensitive and specific • TEE found no vegetations which were overlooked by TTE although vegetation usually better characterized by TEE +San Roman, JA, Vilacosta, I, Zamorano, JL, et al. Transesophageal echocardiography in right-sided endocarditis. J Am Coll Cardiol 1993; 21:1226.
Prosthetic Valve Endocarditis • Findings suggestive of IE in prosthetic valves: • Vegetation • perivalvular abscess and fistula formation • impaired leaflet motion • valve rocking suggesting valve dehiscence • Perivalvular regurgitation. * Must compare to prior. If no, moderate-severe suggestive of IE (not mild) • Echo evaluation can be limited by highly reflective prosthetic materials which block the passage of ultrasound • TEE has higher sensitivity than TTE (82-86% vs 36-43%)13-16 • NPV close to 100% for TEE in native valve endocarditis but not for prosthetic valves making clinical assessment especially important • According to most recent ACC/AHA guidelines, TEE should be first line diagnostic test for possible IE in prosthetic valves
Summary • Echocardiogram part of major criteria in Modified Duke Criteria • Goals to aid in diagnosis, localize vegetations, assess for complications of IE • Mass texture, location, motion, shape, and associated abnormalities important • Vegetation size and mobility correlated with embolic complications in multiple studies • TEE more sensitive than TTE. Both highly specific. • NPV high for TEE. Role for repeat imaging in high risk patients • TEE better at detecting IE complications such as abscess, fistula, and leaflet perforation • TTE = TEE in detecting R sided endocarditis with exception of PV involvement • TEE > TTE for prosthetic valve IE and should be pursued directly • ACC/AHA guidelines from 2006 include recommendations for use of TTE/TEE • Generally TTE is preferred • Class I indications TEE: nondiagnostic TTEs, better assessment of abscess/complications, prosthetic IE • Class IIA indications TEE: persistent staph bacteremia without clear source • ACC/AHA for surgical intervention (severe valve dysfunction, abscess, other penetrating lesion)
References 1. Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1. 2. Bonow, RO, Carabello, BA, Chatterjee, K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008; 118:e523. 3. Role of Echocardiography in Infective Endocarditis. UpToDate. 2010. 4. Shively, BK, Gurule, FT, Roldan, CA, et al. Diagnostic value of transesophageal compared with transthoracic echocardiography in infective endocarditis. J Am Coll Cardiol 1991; 18:391. 5. Mugge, A, Daniel, WG, Frank, G, Lichtlen, PR. Echocardiography in infective endocarditis: reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J Am Coll Cardiol 1989; 14:631. 6. Jaffe, WM, Morgan, DE, Pearlman, AS, Otto, CM. Infective endocarditis, 1983-1988: echocardiographic findings and factors influencing morbidity and mortality. J Am Coll Cardiol 1990; 15:1227. 7. Burger, AJ, Peart, B, Jabi, H, Touchon, RC. The role of two-dimensional echocardiology in the diagnosis of infective endocarditis [corrected] [published erratum appears in Angiology 1991 Sep;42(9):765]. Angiology 1991; 42:552. 8. Pedersen, WR, Walker, M, Olson, JD, et al. Value of transesophageal echocardiography as an adjunct to transthoracic echocardiography in evaluation of native and prosthetic valve endocarditis. Chest 1991; 100:351. 9. Daniel, WG, Mugge, A, Martin, RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991; 324:795. 10. Sochowski, RA, Chan, KL. Implication of negative results on a monoplane transesophageal echocardiographic study in patients with suspected infective endocarditis. J Am Coll Cardiol 1993; 21:216. 11. Shapiro, SM, Young, E, De Guzman, S, et al. Transesophageal echocardiography in diagnosis of infective endocarditis. Chest 1994; 105:377. 12. Birmingham, GD, Rahko, PS, Ballantyne, FD. Improved detection of infective endocarditis with transesophageal echocardiography. Am Heart J 1992; 123:774. 13. Zabalgoitia, M, Garcia, M. Pitfalls in the echo-Doppler diagnosis of prosthetic valve disorders. Echocardiography 1993; 10:203. 14. Daniel, WG, Mugge, A, Grote, J, et al. Comparison of transthoracic and transesophageal echocardiography for detection of abnormalities of prosthetic and bioprosthetic valves in the mitral and aortic positions. Am J Cardiol 1993; 71:210. 15. Alton, ME, Pasierski, TJ, Orsinelli, DA, et al. Comparison of transthoracic and transesophageal echocardiography in evaluation of 47 Starr-Edwards prosthetic valves. J Am Coll Cardiol 1992; 20:1503. 16. Roe, MT, Abramson, MA, Li, J, et al. Clinical information determines the impact of transesophageal echocardiography on the diagnosis of infective endocarditis by the Duke criteria. Am Heart J 2000; 139:945.