Download
1 / 39
390 likes | 410 Views
Learn about how diet influences prenatal outcomes, pollutants linked to birth defects, and regions with poor perinatal outcomes. Understand dietary associations with adverse outcomes like neural tube defects and congenital heart defects.

E N D
Adverse Perinatal Outcomes associated with Environmental and Dietary Factors Phillip V. Gordon MD PhD Elsie Shaefer Chair, Neonatology Assistant Chair of Pediatrics Tulane School of Medicine
What you should get from this talk: • Understand how diet affects prenatal outcomes • There are several pollutants with compelling links to birth defects and/or prematurity • Know which regions of the country have the worst perinatal outcomes (and likely why) • Incorporate this knowledge into your clinical practice and patient counseling
Known Dietary Associations with Common Adverse Perinatal Outcomes • Folate deficiency • Neural Tube Defects • Congential Heart Defects No prenatal vitamins • Cleft Lip and Palate (weak association) Western diet type II diabetes • Congenital Heart Defects • Neural Tube Defects • Small for Gestational Age
Folate Deficiency O2 Free Radicals X Mitochondrial uncoupling increases free radicals and kills stem cells Mitochondrial Uncoupling Particularly vulnerable fetal cell types: neural crest cells & cardiac stem cells
Folate Deficiency & Neural Tube Defects MTRR 66A>G and MTHFR 677C>T are the only two polymorphisms definitively associated with folate metabolism associated with NTDs. However, MTHFR 677C is thought to be prevalent in >½ the world population and a single polymorphism reduces enzymatic efficiency by 50%
What is the evidence that Folate rescues neural tube fusion failure? Meta-analysis for the reduction in NTD occurrence risk observed with periconceptional folic acid supplementation Meta-analysis for the reduction in NTD recurrence risk observed with periconceptional folic acid supplementation x 2 x 5 Folic acid, methylation and neural tube closure in humans. Blom HJ. Birth Defects Res A Clin Mol Teratol. 2009 Apr;85(4):295-302.
The Etiology of Conotruncal Defects The secondary heart field provides myocardium and smooth muscle cells to the arterial pole. Cells of the secondary heart field were labeled at stage 15 (A–D) with a mixture of DiI and rhodamine (red). (A) 4 h after injection at stage 15; labeled cells are located in the ventral floor of the pharynx caudal to the outflow tract. (B) 24 h after injection; labeled cells translocated to the base of the outflow tract. (C) Stage 22 heart 48 h after right secondary heart field injection; left view of the outflow shows labeled cells located in the distal outflow myocardium (arrow) on the left side. (D) Section through outflow of heart in panel (C) stained with anti-rhodamine. Labeled cells are incorporated into the myocardial wall (arrow). Secondary heart field contributes myocardium and smooth muscle to the arterial pole of the developing heart. Waldo KL, Hutson MR, Ward CC, Zdanowicz M, Stadt HA, Kumiski D, Abu-Issa R, Kirby ML. Dev Biol. 2005 May 1;281(1):78-90.
Diabetes and Conotruncal Defects CNC cell migration, apoptosis, and outflow tract septation in Pax3LacZ/1 embryos of nondiabeticand diabetic mice. The approximate area of embryos shown in Figures 1–4 is indicated within the boxed area of the embryo diagram. (A–D) Pax3LacZ/1 embryos were recovered on day 9.5 from diabetic or nondiabeticFVB females that had been crossed with Pax3LacZ/1 males. Embryos were reacted with X-GAL (A,B) to visualize CNC cells, or reacted with a wholemount TUNEL procedure (C,D) to visualize apoptotic nuclei. The fluorescence overlay of a differential interference contrast (DIC) image of the embryos is shown in the insets. (A,C) Pax3LacZ/1 embryos of nondiabetic mice. (B,D) Pax3LacZ/1 embryos of diabetic mice. In image (A) the otic pit is marked by an asterisk, the first somiteis marked by §, and the migrating CNC are marked by arrows. (E,F) Pax3LacZ/1 fetuses were recovered on day 16.5 from crosses of diabetic or nondiabetic FVB females with Pax3LacZ/1 males and cardiac outflow tracts were examined. Images of fetal hearts from (E) nondiabetic pregnancy show the normal outflow tract arrangement, whereas (F) from a diabetic pregnancy show typical outflow tract defects in which the aorta and left pulmonary artery have not correctly separated into distinct vessels (see arrowhead). Oxidative stress during diabetic pregnancy disrupts cardiac neural crest migration and causes outflow tract defects. Morgan SC, Relaix F, Sandell LL, Loeken MR. Birth Defects Res A Clin Mol Teratol. 2008 Jun;82(6):453-63. TruncusArteriosus
Diabetes and Conotruncal Defects CNC migration in embryos following induction of oxidative stress without or with antioxidants. FVB females were crossed with either Pax3LacZ/1 or Pax3GFP/1 males. On day 7.5 of pregnancy, the females were injected with antimycin A (AA) or propylene glycol (PG) as a control. AA-treated pregnancies were also administered GSH-EE on day 7.5, or received supplemental dietary vitamin E succinatebeginning on day 0.5. Embryos were obtained on day 9.5. Pax3LacZ/1 embryos were reacted with X-GAL to visualize CNC migration (A–D), or subjected to a whole-mount TUNEL assay to visualize apoptosis (E–H). Pax3GFP/1 embryos were examined by confocal microscopy (I–L). (A,E,I) Embryos from PG-treated pregnancies. (B,F,J) Embryos from AA-treated pregnancies. (C,G,K) Embryos from AA plus GSH-EE-treated pregnancies. (D,H,L) Embryos from AA-treated pregnancies supplemented with vitamin E. The location of absent CNC cell migration is marked by an asterisk. Arrows point to between the two streams of LacZ- or GFP-positive CNC cells.
What about folate and CHD? Changes in frequencies of select congenital anomalies since the onset of folic acid fortification in a Canadian birth defect registry. Godwin KA, Sibbald B, Bedard T, Kuzeljevic B, Lowry RB, Arbour L. Can J Public Health. 2008 Jul-Aug;99(4):271-5. Conotruncal defects > Non conotruncal defects Conotruncal defects • Non conotruncal defects
What have we learned so far? • Folate deficiency and type II diabetes both exacerbate fetal oxidative stress, which disrupts stem cell proliferation • Polymorphisms in genes that produce enzymes for folate metabolism lead to increased susceptibility to folate deficiency, worsen oxidative stress, and predispose the fetus to NTD or CHD. • The greatest window of vulnerability is during the first 6 weeks of pregnancy (hence the need to take PRENATAL vitamins) • MOST IMPORTANTLY! If you’ve had one child with a NTD or CHD, it is critical that you take prenatal vitamins with folate for the next
Cleft Lip and Palate (CL/P) Nearly all variants of CL/P have now been associated with some form of mutation, deletion or polymorphism within the interferon regulator factor-6 gene. Small effects of diet and smoking have been shown on the incidence of non-syndromic CL/P, likely consistent with effects upon polymorphic susceptibilities. Folate has not reduced the incidence of CL/P. Individuals with various types of orofacialclefting with known and unknown etiologies.
Gastroschisis and Rising Incidence Prevalence of gastroschisis and associated hospital time continue to rise in neonates who are admitted for intensive care. Clark RH, Walker MW, Gauderer MW. J Pediatr Surg. 2009 Jun;44(6):1108-12.
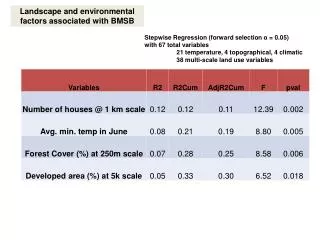
Kelly D. Mattixa, , , Paul D. Winchesterb and L.R. “Tres” Scherera Kelly D. Mattixa, , , Paul D. Winchesterb and L.R. “Tres” Scherera What is causing Gastroschisis? Maternal asthma medication use and the risk of gastroschisis. Lin S, Munsie JP, Herdt-Losavio ML, Bell E, Druschel C, Romitti PA, Olney R; National Birth Defects Prevention Study. Am J Epidemiol. 2008 Jul 1;168(1):73-9. (1) (2) Maternal use of bronchodilators, antiinflammatories, and both and the risk of gastroschisis, National Birth Defects Prevention Study, 1997–2002 Abdominal Wall Defects Indiana Mid West & U.S. Incidence of abdominal wall defects is related to surface water atrazine and nitrate levels. Mattix KD, Winchester PD, Scherer LR. J Pediatr Surg. 2007 Jun;42(6):947-9.
Its not just Gastroschisis… ActaPaediatr. 2009 Apr;98(4):664-9. Agrichemicals in surface water and birth defects in the United States. Winchester PD, Huskins J, Ying J. A statistically significant increased risk was found for any birth defect and also specifically for spina bifida, circulatory, tracheal, gastrointestinal, urogenital, musculoskeletal anomalies, cleft lip, adactyly, clubfoot and Down's syndrome in women with LMPs between April and July in the United Sates
* Adjusted for maternal age, ethnicity, educational level, smoking, folic acid, and any of the following vasoactive medications: aspirin, ibuprofen, acetaminophen, amoxicillin, pseudoephedrine, phenylpropanolamine, and methylenedioxymethamphetamine. * Adjusted for maternal age, ethnicity, educational level, smoking, folic acid, and any of the following vasoactive medications: aspirin, ibuprofen, acetaminophen, amoxicillin, pseudoephedrine, phenylpropanolamine, and methylenedioxymethamphetamine. How does Atrazine cause Birth Defects? It causes Metabolic Syndrome Diabetes Chronic exposure to the herbicide, Atrazine, causes mitochondrial dysfunction and insulin resistance. Lim S, Ahn SY, Song IC, Chung MH, Jang HC, Park KS, Lee KU, Pak YK, Lee HK. PLoS One. 2009;4(4):e5186
Atrazine is also associated with SGA birth Adjusted OR* of small-for-gestational-age status, by the number of months of the third trimester that overlapped with the May–September period Geometric mean of Atrazine levels in raw water by month (μg/l, in the y axis) and lower 95% confidence interval, estimated from an analysis of variance adjusted for year and water distribution unit. Atrazine in municipal drinking water and risk of low birth weight, preterm delivery, and small-for-gestational-age status. Villanueva CM, Durand G, Coutté MB, Chevrier C, Cordier S. Occup Environ Med. 2005 Jun;62(6):400-5.
Following the Atrazine water cycle SGA incidence peaks in the states where Atrazine had the longest windows of effect upon Amphibian birth defects
The Mississippi Delta also has maximum peak exposure because of the water cycle (and so might have a high incidence of birth defects) Watershed Regressions for Pesticides (WARP) Atrazine Model http://infotrek.er.usgs.gov/warp/
Unfortunately, we don’t really have a reliable way to test this hypothesis, because these two states did a poor job of tracking birth defects prior to Hurricane Katrina and things haven’t improved much since healthyamericans.org 2002
Diabetes also maps tightly with SGA Like Atrazine, diabetes can cause both birth defects and SGA births
How does diabetes cause both birth defects and SGA birth? Transcription Change in Response to Diabetes Epigenetic Mechanisms hyperglycemia glycolysis pathway shunting increased free radicals aberrant glycoslation altered methylation and acetylation of glucose transporter promoter sites (life long insulin resistance) free radical disruption of beta cell stem cells (life long insulin resistance and potentiation of diabetes in subsequent generations) oxidative damage from mitochondria, particularly in placenta (ratty placenta leading to SGA) Maternal diabetes alters transcriptional programs in the developing embryo. Pavlinkova G, Salbaum JM, Kappen C. BMC Genomics. 2009 Jun 18;10:274.
Atrazine Concentration (Maximum) Type II Diabetes has dietary risk factors too (and this should be part of our prenatal counseling)
What have we learned now? • Cleft lip and palate is poorly associated with environmental and dietary risks • Gastroschisis incidence has been rising and two environmental risk factors have been associated with this increase: 1) bronchodialators, 2) Atrazine (possibly all triazines) • Atrazine has been temporally associated with a wide number of birth defects as well as SGA births and has been demonstrated to be a mitochondrial inhibitor that induces insulin resistance and metabolic syndrome in rats with low level, chronic dosage (thereby providing a mechanism) • Type II diabetes and SGA birth have close geographic overlap, with Atrazine having the potential to be an important adjunct risk for SGA birth. • Finally, when counseling mothers about all this, we have to remember the basics, like diet, health benefits and risk reduction of breast feeding, and ….
Appropriate hydration using a reliable water source ? OR Water from the bayou Bottled water
Hypospadias Incidence is also Increasing We have to be careful about associations. For example, just because two things go up simultaneously (like sales of bottled water and hypospadias) does not mean they are related in a causal manner.
Phthalates most look like? dibutyl phthalate (DBP) diisodecyl phthalate
Phthalates are everywhere and they do affect humans Phthalates were first introduces in the 1930s as plasticizers Phthalates are associated with decreased urogenital distance and increased incidence of cryptorchidism Increased maternal breast milk concentrations of phthalates are associated with decreased neonatal androgen levels Phthalates have been used to make baby bottles, IV bags, toys, syringes, tubing, containers, pill coatings, piping, building materials and sex toys. They are found literally everywhere in our lives.
= Phthalate Susceptible Pathways during Male Reproductive Tract Development Types of Hypospadias Mullerian Inhibiting Substance Mullerian Duct Regression Glanular Anterior (50%) Sertolli Cell Subcoronal Trans-Abdominal Descent of the Testes Distal Penile INSL3 Leydig Cell Mid- Shaft Middle (30%) Inguino-Scrotal Descent of the Testes Testosterone Proximal Penile Epididymus Vas Deferens Seminal Vescicles 5-alpha reductase Wolffian Duct Differentiation Peno-scrotal Posterior (20%) Genital Tubericle Differentiation Male Genitalia DihydroxyTestosterone Scrotal Urogenital Sinus Differentiation Prostate Gland Perianal (approximately 10% of all hypospadias have undescended testes)
Well, if you can’t drink the water, can you at least breathe the air? Poor air quality has been associated with poor perinatal outcomes: sulfur dioxide, benzene, fine particulate matter associated with car exhaust, and tobacco smoke have all been associated with SGA births Car exhaust has more recently been associated with prematurity and preeclampsia
There is a temporal relationship between car exhaust and preterm birth Five-county metropolitan Atlanta, population density according to the 2000 Census and location of ambient air quality monitoring stations Ambient air pollution and preterm birth: a time-series analysis. Darrow LA, Klein M, Flanders WD, Waller LA, Correa A, Marcus M, Mulholland JA, Russell AG, Tolbert PE. Epidemiology. 2009 Sep;20(5):689-98 Tucker Jefferson Georgia Tech South DeKalb Monitor-specific adjusted risk ratios (circles) and 95% CIs (vertical bars) for preterm birth associated with a 5 ppb increase in NO2 levels in the preceding 6 weeks. Adjusted for long term trends, seasonal trends, race/ethnicity, marital status, education, gestational week and interaction between gestational week and maternal characteristics.
There is a proximity relationship between car exhaust and SGA birth A cohort study of traffic-related air pollution impacts on birth outcomes. Brauer M, Lencar C, Tamburic L, Koehoorn M, Demers P, Karr C. Environ Health Perspect. 2008 May;116(5):680-6.
There is a dose response relationship between car exhaust and prematurity Are we ready for this? Association between local traffic-generated air pollution and preeclampsia and preterm delivery in the south coast air basin of California. Wu J, Ren C, Delfino RJ, Chung J, Wilhelm M, Ritz B. Environ Health Perspect. 2009 Nov;117(11):1773-9.
Poor air quality does not show national geographic parallels to prematurity
Poor air quality does not show national geographic parallels to SGA birth These maps suggest that chronic poor air quality is either not a risk factor or not as great a risk factor as close and chronic proximity to car exhaust
What environmental and dietary risk factors should we really and truly be concerned about in our clinical practice environment? Prenatal vitamins with folate – no brainer, mandatory for a mother who has already had a child with a NTD or CHD (both of which are declining due to folate supplements) *400 mcg before, 600 mcg during pregnancy, up to 1000 mcg for high risk CL/P – probably not environmental or dietary (although vitamins and smoking cessation never hurt anybody). This information can ease maternal guilt. Gastroschisis and hypospadias incidence are rising. Asthmatic mothers need to be in good control to minimize bronchodilator abuse. Well water is probably not a good idea in agricultural or Mississippi Delta regions, especially if they are showing evidence of metabolic syndrome habitus. Phthalate is a concern, particularly if they have an unusual source of exposure (pregnant cancer patient and IV bags). Pregnant women or women planning to get pregnant should avoid plastic products with this sign: Close, chronic exposure to car exhaust is a risk factor for prematurity and SGA birth. It is probably time for us to start asking about living over a garage, working as a mechanic, driving a jalopy with a ruptured manifold, < 50 meters from a highway etc. General exposure, not so much – for now.
Politics is the second oldest profession, scientists separate fact from fiction and clinicians educate the public about their health