Download
1 / 21
210 likes | 247 Views
Unit III: Homeostasis Blood. Chapter 17 pp. 575-585. Review. The most effective buffer in the intracellular fluid is: a.) phosphate; b.) protein; c.) bicarbonate; d.) carbonic acid A blood pH of 7.2 caused by inadequate pulmonary ventilation would be classified as _________.

E N D
Unit III: HomeostasisBlood Chapter 17 pp. 575-585
Review • The most effective buffer in the intracellular fluid is: a.) phosphate; b.) protein; c.) bicarbonate; d.) carbonic acid • A blood pH of 7.2 caused by inadequate pulmonary ventilation would be classified as _________. • Tubular secretion of hydrogen ions would cease if the acidity of the tubular fluid fell below a value called the _________. • (T/F) The bicarbonate system buffers more acid than any other chemical buffer. • Acids ____________ hydrogen ions in a solution, whereas, bases _______ them.
Functions of Circulatory System • Fundamental purpose: transport substances from place to place • Transport • O2, CO2, nutrients, wastes, hormones, and stem cells • Protection • Inflammation, WBCs, antibodies, and platelets • Regulation • fluid regulation, buffering, and heat
Presence of Potassium in Blood Hypokalemia Hyperkalemia Normal potassiumlevels in serum(3.5–5.5 mEq/L) • <2 mEq/L in blood: • muscular weakness • paralysis • >8 mEq/L in blood • cardiac arrhythmias Factors Promoting Hypokalemia Factors Promoting Hyperkalemia Diuretics (Lasix) ↑ volume of urineproduced Kidney failure Aldosteronism overstimulates sodiumretention & potassiumloss Chronically lowbody fluid pH Several drugs promotediuresis by blocking Nareabsorption at thekidneys.
Blood Composition • Adults have 4-6 L of blood • Plasma – • Water, proteins, nutrients, electrolytes, nitrogenous wastes, gases, and hormones (Table 18.2 p. 687) • Serum • Lacks fibrinogen Withdraw blood Centrifuge Plasma (55% of whole blood) Buffy coat: leukocytes and platelets (<1% of whole blood) Formed elements Erythrocytes (45% of whole blood)
Plasma Proteins • 3 major categories of plasma proteins: • albumins - most abundant • contributes to viscosity and osmolarity influences blood pressure, flow and volume • globulins (antibodies) • provide transport, clotting, and immunity • alpha, beta and gamma globulins • fibrinogen • precursor of fibrin help form blood clots • Plasma proteins formed by liver • except gamma globulins (produced by plasma cells)
Formed Elements of Blood • Erythrocytes • Platelets • Leukocytes • Granulocytes • Neutrophils • Eosinophils • Basophils • Agranulocytes • Lymphocytes • Monocytes
Properties of Blood • Viscosity - • whole blood 5 times as viscous as water • Osmolarity (total molarity of dissolved particles that can’t pass through blood vessel wall) • high blood osmolarity • raises blood pressure • low blood osmolarity • lowers blood pressure
Properties of Blood • Hematocrit – (packed cell volume) • Females: 37-48% • Males: 45-52% • pH: 7.35 - 7.45 • RBC count: • Females: 4.2-5.4 million/µL • Males: 4.6-6.2 million/µL • Total WBC count: 5000 – 10,000 /µL • Volume/Body weight: 80-85 mL/kg • Female: 4-5L • Male: 5-6L
Erythrocytes (RBCs) • Disc-shaped cell with thick rim • Gas transport • increased surface area/volume ratio • due to loss of organelles during maturation • increases diffusion rate of substances • 33% of cytoplasm is hemoglobin (Hb) • O2 delivery to tissue and CO2 transport to lungs • Carbonic anhydrase (CAH)
Erythrocytes and Hemoglobin • Common measurements: • Hematocrit (packed cell volume) • Red blood cell count • hemoglobin concentration of whole blood • men 13-18g/dL; women 12-16g/dL • Values are lower in women • androgens stimulate RBC production • women have periodic menstrual losses • Hematocrit is inversely proportional to % body fat
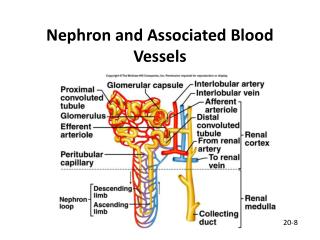
Erythropoiesis • 2.5 million RBCs/sec (hematocrit value of 20mL of RBC/day) • Development takes 3-5 days • reduction in cell size, increase in cell number, synthesis of hemoglobin and loss of nucleus Events Occurring in the Red Bone Marrow Multipotent stem cells Start Proerythroblasts stimulated by erythropoietin (EPO) Erythroblast Macrophages in liver, spleen, and bone marrow Fe2+ transported in circulation by transferrin Fe2+ RBC formation Amino acids Heme Average life span of RBC is 120 days 90% Biliverdin Roughly four days of differentiation Bilirubin 10% Hemolysis Ejection of nucleus Retilculocytes remain in the bone marrow for 2 more days New RBCs released into circulation
Erythrocyte Homeostasis • Negative feedback control • drop in RBC count causes kidney hypoxemia • EPO production stimulates bone marrow • RBC count in 3 - 4 days • Stimulus for erythropoiesis • hemorrhaging, blood loss • low levels O2 • abrupt increase in O2 consumption • loss of lung tissue in emphysema
Anemia • Inefficient amount of red blood cells • Causes: • inadequate erythropoiesis • Kidney failure • Iron-deficiency • Vitamin B12 deficiency • blood loss • RBC destruction • Consequences: • Hypoxia • Decreased blood osmolarity • Decreased blood viscosity
Erythrocyte Disorders • Sickle Cell Disease and Thalassemia • Hereditary Hb ‘defect’ of African Americans and Mediteraneans • recessive allele modifies hemoglobin structure • sickle-cell trait - heterozygous for HbS • individual has resistance to malaria • sickle-cell disease - homozygous for HbS • individual has shortened life • low O2 concentrations sickle shape • stickiness agglutination blocked vessels • intense pain; kidney and heart failure; paralysis; stroke
Antigens and Antibodies • Antigens (agglutinogens) • unique molecules on all cell surfaces • used to distinguish self from foreign • Antibodies (agglutinins) • secreted by plasma cells • Appear 2-8 months after birth; reach maximum at 10 yr. • Transfusion reaction • Agglutination : RBC Antigen-antibody complex Hemolysis Opposing antibodies Surface antigens
ABO Blood Groups • Your ABO blood type is determined by presence or absence of agglutinogens on RBCs and agglutinins in blood plasma. • most common/universal donor - type O • Rarest/universal recipient - type AB Type O Type B Type A Type AB RBCs with both A and B antigens. RBCs with antigen B only. RBCs lacking both A and B antigens. RBCs with antigen A only. Surface antigen B Surface antigen A Plasma contains anti-B antibodies, which will attack Type B surface antigens. Plasma contains both anti-A and anti-B antibodies. Plasma has neither anti-A nor anti-B antibodies. Plasma contains anti-A antibodies.
ABO Group Genetics • A and B alleles are dominant over O; but codominant to each other A AB AB B A B AB B A
Rh Group • 3 antigens: C, D, E • Rh (D) agglutinogens • Rh+ blood type has D agglutinogens on RBCs • Rh frequencies vary among ethnic groups • Anti-D agglutinins not normally present • form in Rh- individuals exposed to Rh+ blood • no problems with first transfusion
Hemolytic Disease of the Newborn Rh– mother Rh– mother First Pregnancy of an Rh– Mother with an Rh+ infant Second Pregnancy of an Rh– Mother with an Rh+ Infant Rh+ fetus Rh+ fetus Maternal anti-Rh antibodies present. These antibodies destroy fetal RBCs dangerous anemia. Need for blood cells ↑ Leave bone marrow under- development. During First Pregnancy Very few fetal cells enter the maternal circulation. Maternal blood supply and tissue Placenta During Second Pregnancy Maternal Fetal blood supply and tissue Maternal antibodies Hemorrhaging at Delivery Exposure to fetal red blood cell antigens generally occurs during delivery. Maternal Fetal Hemolysis of fetal RBCs Rh antigen on fetal red blood cells Fetal Maternal Antibody Production A woman’s first infant is not affected. Maternal antibodies to Rh antigen Maternal
Results of blood typing tests on blood samples from four individuals Blood type Anti-B Anti-D Anti-A A+ B+ AB+ O–