Download
1 / 22
220 likes | 333 Views
How NOT to Perform a First Time, High Risk Evolution. Brian Anderson, DOE-Idaho Nuclear and Safety Performance Division September 13, 2011. Biographical Information – Brian S. Anderson . Employer: U.S. Department of Energy / Idaho Operations Office

E N D
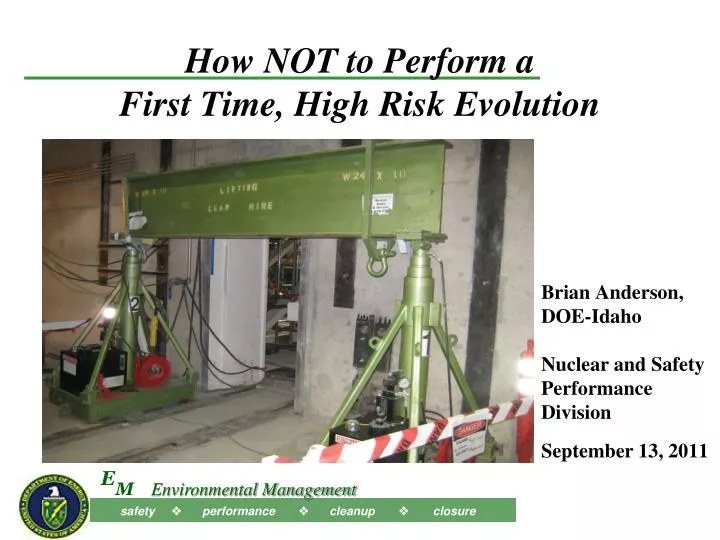
How NOT to Perform a First Time, High Risk Evolution Brian Anderson, DOE-Idaho Nuclear and Safety Performance Division September 13, 2011
Biographical Information – Brian S. Anderson • Employer: U.S. Department of Energy / Idaho Operations Office • Position: Team Leader, Safety Performance Team • Education: BS / Electrical Engineering, U. S. Naval Academy – 1977 • Experience: • 33 Yrs. Nuclear Operations (Submarines, Reactors, Nuclear Facility Operations) • Quality Assurance, ES&H, Construction, Maintenance, Training … • ORR, RA, Accident Investigation, ISMS Verification - Team Lead or member • Certifications: • ANSI/ASME NQA-1 Lead Auditor – 1985, 2009 • U. S. Navy Nuclear Program, Qualified Submarine Officer & Nuclear Engineer 1982 & 1984 • DOE TQP – Senior Technical Safety Manager - 1999
What Happened … • On October 4, 2010 at 0930 hours, workers were up-righting a 7,800 lb. shield door, 104 in. high × 52 in. wide × 30 in. deep • Using a hydraulic telescoping gantry system (HTGS) to support and raise the door into a vertical position • The load shifted causing the door and HTGS to tip • The HTGS’s fall was arrested as the top of the HTGS contacted pipe supports attached to a structural steel I-beam • The shield door came to rest against the pipe supports at about a 15-degree angle from vertical • Three workers were in close proximity, none were injured • Immediate actions taken to isolated and preserve the scene
How it Happened … Work Planning • Work package CWCP # 100145, Install the Concrete Filled Shield Plugs in the 4 Pack (WP), was planned in February 2010 • Engineering did not identify the applicable hoisting and rigging standard for this type of a lifting device (DOE-STD-1090) * … but considered a construction aid • Default determination can be performed as “Skill-of-the-Craft” • However, WP Step 200 is a hold point which requires an engineered lift plan be developed for each door • WP Job Hazard Analysis (JHA) and Job Safety Analysis (JSA) did not identify and mitigate hazards *
How it Happened … Work Planning (Cont’) • URS procurement rented the HTGS and requested certifications for the HTGS … • but did not request an operation/maintenance manual • which was not available during CWCP development • Work package planner did not specify a formal pre-job briefing in the CWCP *
How it Happened … Worker Training • HTGS considered a construction aid, so no training was required * or provided * • "Identify equipment requiring technical expertise for producing acceptable results or precautions for avoiding injury" • "Personnel performing work that requires special skills or abilities shall be qualified and certified prior to performing work.“ • Supervisory and Safety Support staff unfamiliar with HTGS • Superintendents • Field supervisors • General Foremen & Foremen, • Safety personnel, and • Work Package planners • Workers reverted to “Skill of the Craft”
How it Happened … Work Control • A formal process for releasing work to the field is not in place • IWTU work is coordinated using • a plan of the week meeting • a prioritized work list, and • daily meetings where work being done that day is discussed • Both ironworker and millwright superintendents not at work • At the daily meeting, no oversight of the HTGS activity was specified (complex equipment and first-time use) * • Construction manager/superintendent and general foreman / foreman did not review the work packages daily * 6
How it Happened … Work Control (Cont’) • Work activity pre-job brief was LTA • Construction Engineer / General Foreman / Foreman conducts * • with all stakeholders (users, craft, supervisors, & support staff) * • to review every part of the work package * • to ensure a thorough understanding of the job * • WP not checked out for use at the work site * • and not reviewed by personnel at Pre-job briefing* • and not used to control the work • resulting in a missed hold point - rigging engineer prepare lift plan * 7
How it Happened … Management & Oversight • Emphasis on schedule exceeded emphasis on methods • Schedule pressure lead to “Get it Done” mindset • Supervision oversight was less than adequate • Superintendent not familiar with use of the HTGS • Foremen and supervisors not familiar with use of the HTGS • Safety personnel not familiar with use of the HTGS • Improvement in using work documents in the field as a result of corrective actions taken in May of 2010 • OE at IWTU has shown an increased potential for errors for first time evolution/equipment use, Cranes & “Skill-of-the-Craft” • April 2008 dropped Crane Jib boom • April 2009 dropped butt section of the crane boom
Task execution errors in … Use of WP to control work * No lift plan * Cross bar leveling, Free travel of the towers, Centering load on the cross bar between the towers, and Use of the Hilman rollers. Failure to “Step back” when questions arose * Ironworker Foreman not familiar with WP use Posted operating instructions on the HTGS were not used or followed: NOTE statement directs the operator to ensure the gantry is free to center itself over the load during the lift How it Happened … Task Execution 9
Lift Execution • The HTGS was received, assembled and functionally checked using “Skill-of-the-Craft” • The specification sheet provided by the equipment owner was available and used • Two Hillman rollers were set under the opposite end of the door to allow the bottom of the door to roll as needed • Millwright foreman conducted a pre-job brief w/millwrights and iron workers even though ironworkers performed lift • did not identify the hazards or training & operating requirements • The iron workers decided to chock the wheels using wood wedges, ½-in. plywood & small metal plates
Lift Execution (Cont’) • Attached a come-a-long from bottom of door to building structural column to control door movement • Stationed workers to operate come-a-long and adjust rollers
Lift Execution (Cont’) • Stop periodically to tap the east Hillman roller into alignment • Observer gave the door end a push to be sure it was moving • Visually determined if the cross beam on the HTGS was level* • Stopped the lift few times to re-level the HTGS cross beam
Lift Execution (Cont’) • When the door reached vertical, the center of gravity of the door shifted South away from the line between the Hillman rollers and the slings to the center of the door
Gantry Truck Diagram 5 Top View of Setup Just Before Incident Cross Beam Hilman Rollers Shield Door Come a long Operator Tail Line 3rd Iron worker HTGS Operator Gantry Truck N Lift Execution (Cont’)
The Event … • As the door reached vertical, it rocked through the HTGS uprights (towers) and slightly to the South • At the same time the East Hillman roller appeared to stop • HTGS moved 1 to 2 ft to the South and East, tipping and contacting the structural steel I-beam • Door stopped by Unistrut supporting conduit and cables • The iron worker operating the HTGS retreated to the West • The iron worker operating the come-a-long on the South noticed the tipping and pushed the 3rd iron worker, by the South end of the shield door, to the West and followed him out of the way
Suggested Actions for LL Program Improvement – Complex-wide
Corrective Actions 33 Corrective Actions Developed Examples: • Changed work control • Trained on equipment and validate training • Supervision present for first time events • O&M manual present for all lifting equipment • Retrain crafts on need for CWCP in field
What Do You Think… ? • Could this happen at your site? • How does work as performed compare with work as imagined? • What should have been done to prevent this? • Agree with Causal Analysis? • Corrective Actions appropriate? 20
Preventing an Accident is the best thing you’ll never realize you did • It’s better to Prepare and Prevent than to Repair and Repent • If we do this right, there may be dozens of accidents that were prevented • We’ll never really know what they were, because they didn’t happen • It doesn’t happen by “Accident” • A questioning attitude needs cultivated • Organizational learning must be embraced • Safety must undergo constant examination • Examine :Work as Performed” vs. “Work as Imagined” • Start “ Preventing Accidents”