Download
1 / 16
240 likes | 884 Views
SULFONAMIDES. Infectious Diseases Hussain Talal Bakhsh King Abdul Aziz University Faculty Of Pharmacy. Outline. Introduction Mechanism of action Antibacterial Spectrum: Pharmacokinetics Indication ADR PregnancyLactation Administration & Dosage Patient counseling Reference.

E N D
SULFONAMIDES Infectious Diseases Hussain Talal Bakhsh King Abdul Aziz University Faculty Of Pharmacy
Outline • Introduction • Mechanism of action • Antibacterial Spectrum: • Pharmacokinetics • Indication • ADR • Pregnancy\Lactation • Administration & Dosage • Patient counseling • Reference
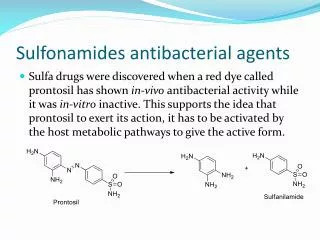
Introduction • The sulfonamides are synthetic bacteriostatic antibiotics with a wide spectrum against most gram-positive and many gram-negative organisms. • However, many strains of an individual species may be resistant.
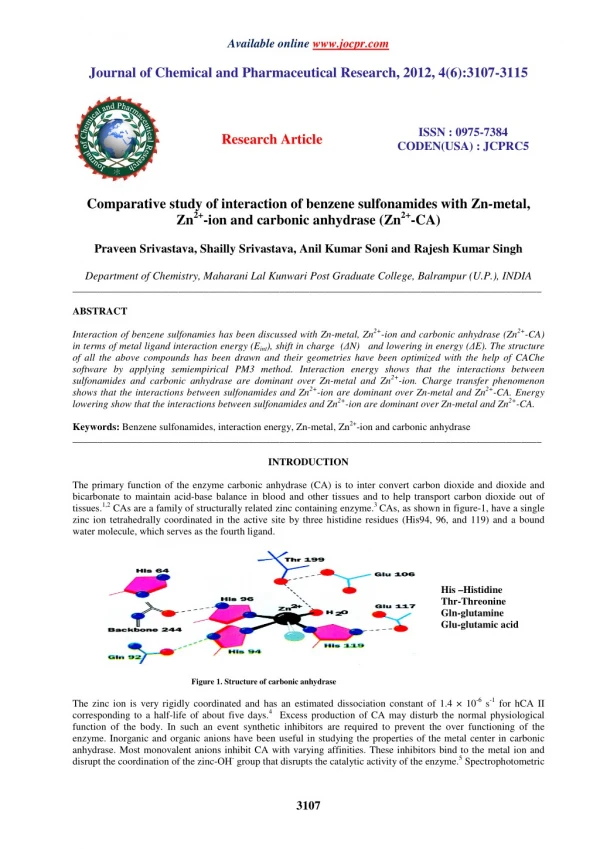
A- Mechanism of action: Many bacteria must rely on their ability to synthesize folate from PABA. In contrast , human beings cannot synthesize folic acid and must obtain performed folate as a vitamin in their diet. Because of their structural similarity to PABA, the sulfonamides compete with this substrate for the enzyme dihydropteroate synthetase, thus preventing the synthesis of bacterial folic acid ( Coenzymes are required for synthesis of purines and pyrimidines) , resulting in inhibition of RNA & DNA synthesis. In absence of folic acid cells cannot grow or divide.
B- Antibacterial Spectrum: Sulfonamides are active against gram +ve cocci ( staph. & strepto.) & bacilli (Clostridium tetani). Also, sulfas active against gram –ve cocci ( Neisseria gonorrhoeae) & Bacilli (E.coli).
C- Pharmacokinetics: Absorption:Most sulfonamides are readily absorbed orally. However, parenteral administration is difficult, since the soluble sulfonamide salts are highly alkaline and irritating to the tissues. Distribution: The sulfonamides are widely distributed throughout all tissues. High levels are achieved in pleural, peritoneal, synovial, and ocular fluids. Although these drugs are no longer used to treat meningitis, CSF levels are high in meningeal infections. Their antibacterial action is inhibited by pus.
Metabolism: Primarily in liver. The product is devoid of antimicrobial activity, but it retains the toxic potential to precipitate at neutral or acidic pH, causing Crystalluria ( stone formation ) , leading to kidney damage. Excretion : Excretion is primarily renal by glomerular filtration with minimal tubular secretion or reabsorption.
D- Indications: • Oral Absorbable (eg. sulfamethoxazole) • • Urinary tract infections (infrequently used alone) • Oral Nonabsorbable (eg. sulfasalazine) • • Ulcerative colitis, inflammatory bowel disease • • Metabolized by gut microflora • • Metabolites are anti-inflammatory • Topical (eg. sulfacetamide) • • Bacterial conjunctivitis (pink-eye) • • Infections resulting from burns or wounds • in combination with pyrimethamine in the treatment of toxoplasmosis, • as a substitute for penicillin in prophylaxis of rheumatic fever .
E- Adverse Effect: 1- Crysalluria. 2- Hypersensitvity. 3- Hemolytic anemia :with G6PD deficiency. 4- Kernicterus : occur in new born because sulfas displace bilirubin from binding site on serum albumin. 5-Drug potentiation :with tolbutamid or wafarin. 6-Stevens-Johnson syndrome: • occurs in < 1 % of treatment courses • skin and mucous membrane eruption
F-Sulfonamide Resistance • 1. Decreased permeability to sulfonamide • 2. Lack dihydropteroate synthase • 3. Mutation resulting in ↑↑ PABA synthesis • 4. Mutation in dihydropteroate synthase so sulfonamide can not bind
G- Pregnancy\Lactation • Avoided in newborn & pregnant women. • When these drugs are given in pregnancy, high levels are achieved in the fetus -------> Kernicterus
H-Administration and Dosage • Systemic sulfonamides:An initial loading dose is commonly recommended but is unnecessary and should not be used in treating UTI (the major use for sulfonamides). It is rarely needed for most other indications. • Sulfisoxazole is used in a dosage of 1 g q 4 to 6 h po in adults. (If a loading dose is used, it is 2 to 4 g.) In children, 150 mg/kg/day is given orally in 6 divided doses; the loading dose if used is 75 mg/kg. • Sulfamethoxazoleis used orally in a dosage of 1 g bid to tid in adults and 25 to 30 mg/kg bid in children. (Loading doses are 2 g in adults and 50 to 60 mg/kg in children.) • Sulfadiazine is used in the same doses as sulfisoxazole. Sulfamethizoleis used in a dosage of 500 to 1000 mg tid to qid in adults and 30 to 45 mg/kg/day in 4 divided doses in children. • Topical sulfonamides: Silver sulfadiazine and mafenide are used topically to prevent infection in burns. Sulfacetamide is useful in treating ocular infections.
I-Patient counseling • To avoid crystalluria and renal damage, fluid intake should be sufficient to produce a urinary output of 1200 to 1500 mL/day. • Sulfonamides should not be used in renal insufficiency.
References • Chambers HF. Sulfonamide, Trimethoprim, & Quinolones. In: Katzung BG. Basic & Clinical Pharmacology. 9th ed. Columbus, OH, USA: McGraw-Hill; 2004; chapter 46: pp. 773- 775. • http://www.merck.com/mrkshared/mmanual/section13/chapter153/153i.jsp • http://w3.ouhsc.edu/cell_biology/AHPharmSyllabus05/Chemotherapy%20Overview%20-%20Reinke05.pdf • http://www.ovc.uoguelph.ca/BioMed/Courses/Public/Pharmacology/pharmsite/98-409/notes/Kalisch/sulfonamides.pdf