Download
1 / 51
530 likes | 1.31k Views
Bundled Payments. Stephanie Cain, APN, DNP Advanced Practice Nurse - Colorectal Center UnityPoint Health Peoria- Methodist Medical Center. Stacey Schulz, MBA Sr. Contract Manager UnityPoint Health - Meriter. Bundled Payments. Purpose & Learning Objectives.

E N D
Bundled Payments Stephanie Cain, APN, DNP Advanced Practice Nurse - Colorectal Center UnityPoint Health Peoria- Methodist Medical Center Stacey Schulz, MBA Sr. Contract Manager UnityPoint Health - Meriter
Bundled Payments Purpose & Learning Objectives • Give an overview of Bundled Payment initiatives at UnityPoint - Meriter and UnityPoint- Peoria Methodist • What are Bundled Payments? • How do we structure a Bundled Payment Program? • What is impact of Bundled Payments on delivery of Care?
Bundled Payments Fee For Service Payments • Separate payments for each service during a single illness or course of treatment • Fragmented provision of care • Minimal coordination across providers and health care settings • Rewards quantity vs. quality
Bundled Payments What are Bundled Payments? • A lump sum payment for an entire episode of care • More coordinated care • Higher quality outcomes • Lower cost to payors/patients • Opportunity to align incentives for providers across the care continuum
Bundled Payments Available Opportunities • Partnership for Healthcare Payment Reform – Private Payor Bundle Pilot • Center for Medicare and Medicaid Innovation (CMMI)’s Bundled Payments for Care Improvement Initiative (BPCI)
Bundled Payments PHPR • Initiative sponsored by the Wisconsin Health Information Organization: provide superior healthcare at affordable costs • Total Knee Replacement Pilot • Bundled Payment with a private payor • Collaborative communication and feedback amongst participants (providers and payors) • Ability to design episode of care and required performance measures
Bundled Payments CMMI – Bundled Payments for Care Improvement Initiative • Four innovative payment models • Financial and performance accountability measures • Care redesign/enhancements • Evidence-based medicine • Standardized operating protocols • Improved care transitions • Potential to gainshare
Bundled Payments : CMMI BPCI Models of Care • Model 1: Retrospective Acute Care Hospital Stay Only • Model 2: Retrospective Acute Care Hospital Stay plus Post-Acute Care • Model 3: Retrospective Post-Acute Care Only • Model 4: Prospective Acute Care Hospital Stay Only
Bundled Payments: Model 2: Retrospective Acute Care Hospital Stay plus Post-Acute Care • 48 Episodes (MS-DRG severity family) to select from Post-Acute Episode Length • 30, 60, or 90 days • 3% discount for 30 and 60 days • 2% discount for 90 days • Risk Track for Outliers • A: 1/99, B: 5/95, C: 5/75 • Responsible for 20% of episode payments above the high-end threshold • Model 2 Waivers • Payment Policy Waivers • 3-Day Stay Requirement for SNF Payment • Post-Discharge Home Visit • Telehealth • Fraud and Abuse Waivers • Savings Pool Contribution Waiver • Incentive Payments Waiver • Group Practice Gainsharing Waiver • Patient Engagement Incentive Waiver
Bundled Payments: BPCI Model 2 - Meriter • Major joint replacement of the lower extremity MS-DRG 469: Major joint replacement or reattachment of lower extremity with major complication or comorbidity MS-DRG 470: Major joint replacement or reattachment of lower extremity without major complication or comorbidity • 90 days, 2% discount • Risk Track B (5/95) • Fraud and Abuse Waivers • Savings Pool Contribution Waiver • Incentive Payments Waiver • Group Practice Gainsharing Waiver • Live: January 1, 2014
Bundled Payment CMS Pricing Rules
Bundled Payments Post-Episode Spending • CMS will perform a Post-Episode Spending Calculation for the 30-Day Post-Discharge period after an episode ends • Total expenditures during the 30-Day Post-Episode period exceeding the Risk Threshold (5/95), is excess spending that must be repaid.
Bundled Payments Net Payment Reconciliation Amount
Bundled Payments Opportunity to Gainshare • Model 2 Fraud and Abuse Waivers allow the development of a Gainsharing Program to allow Awardees to share savings with providers/practitioners involved in Care Redesign for identified Episodes of Care • Internal Cost Savings • Positive Net Payment Reconciliation Amounts
Bundled Payments: Gainsharing Program Requirements • Ensure care is not inappropriately reduced • Maintain or improve quality of care • No inappropriate change in utilization or referral patterns • Protect against fraud, waste, and abuse
Bundled Payments Bundled Payment Process • Convene an interdisciplinary team • Define the episode of care • Develop performance measures • Financial • Quality • Create model of care • Price the episode of care • Identify cost reduction opportunities • Develop gainsharing program • Foster a continuous process improvement plan
Bundled Payments Interdisciplinary Team • Designed to develop and monitor the episode of care and performance • Legal/Policy • Clinical Leaders: inpatient, surgical, therapy, post-acute care • Quality/Performance Improvement • Finance/Data analysis • Administration • Physicians
Turning Physician Interest into Engagement Monthly Meetings We Demonstrated Solidarity We Asked for Help We Brought Data For the first time, physicians were able to see how they were performing not only as an individual, but also relative to their peers. We were transparent. Throughout the course of the meetings, we asked for the physicians to help us design the bundle. We included them in the process. Physicians walked into a room with a room full of administrative and operational power. We were committed.
Bundled Payments Define the Episode of Care • Define episode parameters • Included services and items • Excluded services or items • Related Post-Acute Care • Length of Episode • Qualification Criteria • Eligibility criteria • Ex: Age, limitations of co-morbidities, etc. • Outlier Protection • Understand where outlier risk resides • Episode development and model of care manages clinical risk not probability risk
Bundled Payments Develop Performance Measures • Aim to balance cost and quality outcomes • Complete analysis of “baseline” cost of episode of care • “Cost” defined as real cost • Segregate variable cost to model volume risk • Assign Target Cost for purposes of gainsharing (if applicable) • Determine quality measures • Revision rates • Pain scores • Patient satisfaction scores • Return to functionality assessments (KOOS/WOMAC)
Bundled Payments Monitoring and Tracking Data • Develop a mechanism for tracking data • Systematize processes • Communicate outcomes and results timely • Question outliers and idiosyncrasies • Learn from them and adjust processes, screenings, communications, etc. accordingly • Consider sample size • Need an “n” that is significant
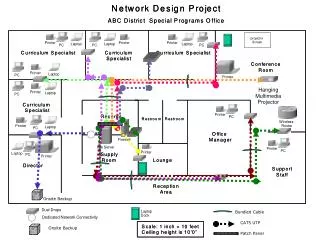
Data Analysis Challenge: Linking Disparate Data Acute-Stay/ Discharge Post-Acute Care Surgery Pre-admission Supply/ Purchasing Records Physician Clinic Records Home Health Records Inpatient Stay Records OR Records Pharmacy Records Insurance Records Anesthesia Records Quality Records Therapy Records Records that are owned by other entities
Bundled Payments Create Model of Care • Identify standards of care and best practices • Understand the cost variation for each component of service • OR • Implant • Inpatient • Therapy • Home Care • SNF • Readmissions • Facilitate conversations to identify opportunities by comparing peer-to-peer and against best practice guidelines • Share data and let the data speak for itself • Identify physician champions • Solicit supporting documentation/educational articles, etc.
Pre-bundle Patient Care Surgery/ Acute Stay Post-Acute Care Pre-admission Discharge
Post-bundle Patient Care Surgery/ Acute Stay Post-Acute Care Pre-admission Discharge The Value of Working Across a Continuum of Care: • Growing partnership for all stakeholders throughout patients’ continuum of care • Increased physician and nursing collaboration to ensure quality care • Increased focus on practicing evidenced-based care • Improved coordination of care with internal and external stakeholders • Increased focus on appropriateness of post-acute care • Increased stakeholder awareness for how to deliver high quality, lower cost care
Bundled Payments Price the Episode of Care • Define baseline/target price for bundle • CMMI factor in discount • Private payor factor in margin • Assess outliers • CMMI Risk Track • Provision for outliers with private payor or manage risk with eligibility criteria • Prospective vs. Retrospective • Prospective requires distribution of payments to episode of care providers • Retrospective requires reconciliation and settling • Determine frequency of analysis and reconciliation to settle and close episodes
Bundled Payments Identify Cost Reduction Opportunities • Understand the detailed cost for each component of the bundle • Review standardization opportunities • Major: anesthesiology method • Minor: updating physician preference card • Define key cost components to monitor and track • Inpatient Costs • Surgical Costs • Implant Costs • Sum of Variable Costs • Readmission • Emergency Room • Skilled Nursing Facility • Home Health • Outpatient Therapy
2012 Meriter Discharge Data (MS-DRG 470) • Nationally, Medicare Post-TKA SNF discharge rates average between 37-45% • SNF discharge percentages highly variable across Meriter orthopedic providers (11% to 71%) • A recent inpatient chart review of 15 PPIC patients discharged to Skilled Nursing Facilities revealed the following: • 7 of the 15 patients reviewed had mobility limitations or lack of support at home that met skilled criteria for SNF admission • 8 of the 15 patients were transferring and ambulating without physical assistance prior to acute care discharge and had a spouse or other caregiver available to provide support. Questionable whether skilled criteria met.
Bundled Payments Meriter’sGainsharing Mechanism • Group Circuit Breakers • Eliminate payment to the whole group if quality materially declined • Individual Circuit Breakers • Eliminate individual physician’s payment if defined performance measures are not met, or materially declined
Bundled Payments Gainsharing Mechanism • Required Savings • 3% CMS Target Price • Allows coverage for administrative costs • Additional Savings to be shared 50% with Hospital and 50% with Physicians • Qualifying Cases • Payouts are determined based on number of qualified cases • Qualifications are based on criteria and standards set by the group • Pain Management • Implants • LOS • OR efficiency, etc. • Physicians can make the best decision for an individual patient and may lose a portion (qualified case) of gain-sharing but is not automatically forfeiting any incentive for the period
Bundled Payments Foster Continuous Improvement • Quarterly Interdisciplinary Team Meetings • Report Outcomes • Review Variances • Introduce Ideas or Opportunities • Performance Dashboard • Ongoing review and response to variances or changes in cost or quality data • Open communication and discussion of industry articles and research
Bundled Payments Online Guided CarePath: Wellbe.me
Bundled Payments Private Payor Considerations • Ability to develop contractual provisions • Compliance • Termination • Available and applicable waivers • Claims processing • Applicable restrictions
Bundled Payments CMS Bundled Payment Initiative UnityPoint Health Peoria Methodist Medical Center • Methodist has selected to be paid a bundled rate for major bowel procedures which includes DRGs 329, 330 and 331. (colon resection primary) • Under the bundled payment initiative, Part A & B services are bundled beginning on the first three days prior to hospital admission through 90 days post discharge. • Providers continue to bill Medicare under fee-for-service. At the end of each contract year, a retrospective reconciliation occurs against the target price. • Methodist selected Risk Tract 2 and launched Oct 1, 2013 • Methodist is also a medical shared savings participant with 11,000 attributed members.
Bundled Payments Methodist Triple Aim Objectives • Improve clinical outcomes of bowel resection patients. • Coordinate patient care across the continuum to reduce readmissions, unnecessary testing, and patients adherence to recommended care. • Improve the patient’s experience as measured by HCAHPS scores. • Increase physician satisfaction through participation in the care redesign process, outcome measurement and economic alignment. • Improve operating efficiency resulting in lower costs.
Bundled Payments Peoria Bundle Components • Home health agency services (HHS) • Hospital outpatient services • Independent outpatient therapy services • Clinical laboratory services • Durable medical equipment • Part B drugs • Physicians’ services • Inpatient hospital services (episode anchor) • Inpatient hospital readmission services • Long term care hospital services (LTCH) • Inpatient rehabilitation facility services • Skilled nursing facility services (SNF)
Bundled Payments Private Payor Considerations • Ability to develop contractual provisions • Compliance • Termination • Available and applicable waivers • Claims processing • Applicable restrictions
Top Initiatives to support project • Started engaging surgeons 5 months before project started • Weekly meetings; data; 1:1 meetings • Shared baseline data early on so all new current situation and opportunity • Included in design of gain share model, metrics, and dashboard design • Saw need to hire colorectal NP navigator (dual role Bundled project and launch colorectal cancer center) • Invested time in gaining surgeon consensus on order sets, processes and procedures
Top Initiatives to support project • Engaged wide stakeholder groups • Nursing units • Administration • PI analyst • Finance • Case management • Coders • OR staff • Schedulers • Surgeon office staff • Primary care providers • LTC’s
Positive Outcomes • Good engagement from surgeon groups • Good awareness and adherence to processes sets from OR and nursing staff • OR staff asking about opening expensive items • Nursing staff and getting patients moving quicker and setting discharge expectations
Positive Outcomes • Internal cost savings being achieved • ICU LOS and overall LOS down • Cost per Case down (supplies in OR) • Decreased Surgical Site Infection • Navigator working well • Patients like having navigator at the hub • Surgeons like navigator to round and provide updates and recommendations
Lessons learned and opportunities for growth • Major Bowel Procedures might not be the best to start with? • Challenges • Identification/Coding • Surgeon called in to minor assist and it gets coded as bundle despite “not theirs”- perforated bowel • Inclusion & Exclusion Criteria • Elective vs. Emergent Cases and no pre-op screening and mitigation • Would have hired the NP earlier
Lessons learned and opportunities for growth • Consensus takes time related to various surgeon practice preference related to training and beliefs • Example- standardized antibiotic use, close vs. open decisions, use of wound vacs, how soon to do surgery vs. wait • Surgeons who are on the bundled team are very engaged…they are not so good at getting the processes and information to their peers • Requires going to offices periodically to review data metrics, and gain sharing • Keeping them engaged is helps to have citizenship as part of gain share.
Miscellaneous • What/How is critical to helping manage? • Nurse Practitioner, PI, Case Managers • What’s missing or challenging? • Sometimes hard to know in the bundle or not? • Patients presenting in crisis so poor outcomes • Not able to take advantage of the SNF waiver due to the nature of the surgery not being 3 day initial LOS and not doing any direct admits post op at this time due to so few readmits that would be stable