Download
1 / 43
450 likes | 790 Views
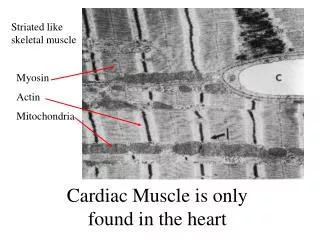
Cardiac Muscle is only found in the heart. Striated muscle cells with T- tubules on the Z lines 1 T-tubule per sarcomere Skeletal muscle which is faster has 2 per sarcomere. Cells contract in response to an action potential (like skeletal muscle).

E N D
Striated muscle cells with T- tubules on the Z lines 1 T-tubule per sarcomere Skeletal muscle which is faster has 2 per sarcomere Cells contract in response to an action potential (like skeletal muscle)
Many mitochondria. With aerobic metabolism of FFA and Lactate Only ~15% of metabolism is glucose
There are no motor nerves or end plates in the heart The beat originates in the cardiac muscle itself. The heart beat is therefore called myogenic (muscle + origin) Skeletal muscle is Neurogenic
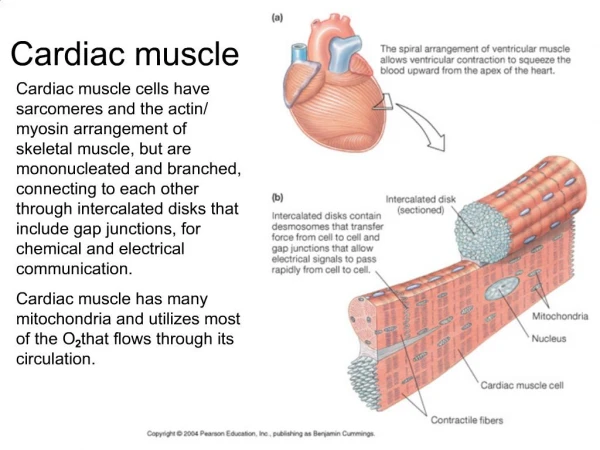
Cells are rich in Gap Junctions at the intercalateddiscs Action potentials are conducted from cell-to- cell through the gap junctions causing every cell in the heart to contract with each beat. The heart is said to act as a functional syncytium (single cell) even though composed of individual cells
Desmosomes transmit mechanical force from cell-to-cell. They are sort of “molecular rivets”
Specialized cardiac muscle types 1. Contractile (found in the Atrium and Ventricle). 3. Conductile (specialized to conduct quickly: Purkinje cells) 4. Nodal (specialized to act as pacemakers or conduct very slowly as in the AV node).
Phase 0 is the rapid spike due to increased Na+ conductance (it is regenerative thanks tovoltage-gated fast sodium channels). Phase 1 is the recovery from the overshoot due to closure of Na+ channels and transient opening potassium channels, Ito.
Phase 2 is the plateau Due to Ca++ influx through slow (L-type) calcium channels. They are called slow because they stay open for about 300 ms Prolongs the action potential to 300 ms to maintain force generation and create a long refractory period (see below)
Phase 3 The repolarization phase is due to increased potassium conductance. Two channel types open, IK (delayed rectifier) and IK1 (inward rectifier) Phase 4 is the resting potential between beats.
Like skeletal muscle mechanical contraction lags behind the action potential.
Absolute refractory period: all inactivation gates are closed no electrical stimulus will elicit another action potential. Runs from phase 0 through most of phase 3. Because of the refractory periods heart muscle cannot be tetanized. Relative refractory period: some inactivation gates are open. An action potential can be elicited but a higher stimulus voltage is required and not all channels participate.
Absolute Supranormal period: The cells can be restimulated and the threshold is actually lower than normal. Occurs early in phase 4 as some potassium channels close. S.N. Rel This can be source of reentrant arrhythmias especially when phase 3 is delayed as in long Q-T syndrome as their positive afterpotentials fall in the supranormal period and can trigger another action potential.
+ K ATP Pump Ex + ++ Na + Ca Na Some calcium enters the cell through the slow Ca++ channels during phase 2. This is called Trigger Ca++. Trigger Ca++ binds to the ryanodine receptors on the sarcoplasmic reticulum (SR). Extracellular Fluid ++ Ca Sarcolemma L type channel Cytosol ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments
+ K ATP Pump Ex + ++ Na + Ca Na Most of the calcium that activates the muscle comes from the SR. This is termed calcium-induced calcium release. The Ryanodine receptors are actually Ca++ channels. Calcium binding causes them to open and release Ca++ that is stored in the SR Extracellular Fluid ++ Ca Sarcolemma L type channel Cytosol ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments
+ K ATP Pump Ex + ++ ++ Na + Ca Ca Na After the action potential subsides calcium is pumped back into the SR by a calcium ATPase,called SERCA. Extracellular Fluid ++ Ca Sarcolemma L type channel Cytosol ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments
Much of the calcium stored in the SR is bound to calsequestrin thus increasing the SR’s capacity. Ca++ has low solubility and would precipitate in the SR without casequestrin.
Calcium is moved out of the cell by the Na/Ca exchanger. To maintain a steady state as much Ca++ leaves the cell over one cycle as entered. The exchanger gets its energy from the sodium gradient. A small amount of calcium is also pumped out by a sarcolemmal calcium ATPase (pump) Extracellular Fluid ++ Ca + K Sarcolemma ATP Pump Ex L type channel Cytosol + ++ Na + Ca Na ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments
Insufficient Ca++ is released with each action potential to cover all troponin binding sites. Therefore increasing the cytosolic calcium concentration increases the force of contraction.
Extracellular Fluid ++ Ca + K Sarcolemma ATP Pump Ex L type channel Cytosol + ++ Na + Ca Na ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments Decreasing the sodium gradient by the sodium pump inhibitor digitalis causes less calcium to leave via the exchanger and consequently more to enter the SR. That increases force of contraction
Hearts are very sensitive to serum Ca++. Low serum calcium results in loss of trigger calcium, low SR calcium and a weak heart beat The strength of the beat is proportional to the amount of calcium stored in the SR. SERCA competes with surface exchangers for Calcium during phase 4 and anything that promotes more calcium in the SR increases the force of contraction.
Increasing the heart rate causes more calcium to enter per unit time and decreases time spent in phase 4. This causes Ca++ to accumulate in the SR. Hence increasing the heart rate increases force of contraction
Extracellular Fluid ++ Ca + K Sarcolemma ATP Pump Ex L type channel Cytosol + ++ Na + Ca Na ++ Ca Trigger ATP SERCA ++ Ca Sarcoplasmic reticulum Ryanodine receptor Sliding filaments Blocking L-Type Calcium channels with nifedipine a dihydropyridine reduces calcium entry with each beat and reduces contractile force.
SERCA which pumps Ca++ back into the SR is modulated by Phospholamban. Increasing SERCA activity will increase the force of contraction because SR will contain more calcium Protein kinase A (PKA) phosphorylates both L-type Ca++ channels (opens them) and Phospholamban which in turn increases SERCA activity
Opening the L-type Calcium channel brings more calcium in with every beat.
Phosphorylating phospholamban causes SERCA to pump more calcium in the SR.
Phosphorylating troponin I decreases its calcium affinity causing the muscle to relax faster (lusitrophic effect).
How can we vary the force of contraction in any striated muscle? • Increase the duration of the active state (skeletal only) • Increase muscle length • Increase contractility (cardiac only)
In skeletal muscle the force generated by a single action potential (twitch) is very small. Force is increased by repetitive stimulation and fusing action potentials together (prolonging the active state). In cardiac muscle every beat is a twitch with a long refractory period. Temporal summation is not possible
Skeletal muscle AP The plateau prolongs the active state in cardiac muscle so that full tension occurs with a single twitch.
How can we vary the force of contraction in any striated muscle? • Increase the duration of the active state (skeletal only) • Increase muscle length • Increase contractility (cardiac only)
Change the resting muscle length (preload). As in skeletal muscle the force of contraction is very dependent on the geometry of the overlap between the thick and thin filaments Starling’s law of the heart: The more the heart is filled during diastole the more forcefully it will contract during systole
The top figure is actually for skeletal muscle because the relaxed tension is still zero at the peak of the contracted curve (Lo). Contrast that to the curve in in the lower panel. The high passive tension opposes over-filling of the ventricle during diastole.
How can we vary the force of contraction in any striated muscle? • Increase the duration of the active state (skeletal only) • Increase muscle length • Increase contractility (cardiac only)
Change the contractility A change in contractility is defined as a change in force of contraction not related to a change in length. A change in contractility can be seen as a shift in the “contracted” curve either up (an increased contractility) or down (a decreased contractility)
Sympatheic nerve activity is the usual cause of an increased contractility. Heart failure occurs when contractility is pathologically reduced Contractility is hard to measure in patients
Isotonic contraction is where the tension is held constant and the muscle is allowed to shorten The higher the contractility the more blood will be ejected The heart contracts in an isotonic manner 4. Contraction Aortic pressure Total 3. At this point the ventriclebegins to eject and the contraction becomes isotonic stops here 125 100 2. Isometric contraction as pressure builds 75 stroke Pressure (mmHg) 1. The ventricle is filled volume 50 25 Resting 20 40 60 80 100 Volume (ml)
The greater the load the slower the muscle shortens If the length is increased at any load the speed of shortening increases The force-velocity curve can be extrapolated to zero force to determine the maximum velocity of shortening,Vmax. Notice that Vmax is the same at all lengths
Changes in contractility shift the entire curve including the y axis intercept, Vmax Vmax is a length-independent index of contractility. Unfortunately Vmax is hard to measure in humans
Optimal load Power = force x velocity. The power generated by the heart is a function of its load. Note that there is an optimal load.
There is a tendency for students to treat length tension diagrams as specific for isometric muscles and and force-velocity plots as specific for isotonic muscles. Actually they are just two sides of the same coin.