Download

1 / 26
300 likes | 526 Views
Bilirubin metabolism and jaundice. Objectives. Bilirubin metabolism and pathophysiological mechanism. Bilirubin uptake and transport. Jaundice condition and types. Pathophysiological importance of bilirubin metabolism. It is the end product of heme degradation.

E N D
Objectives • Bilirubin metabolism and pathophysiological mechanism. • Bilirubin uptake and transport. • Jaundice condition and types.
Pathophysiological importance of bilirubin metabolism • It is the end product of heme degradation. • Serum bilirubin level is an important clinical marker of hepatobiliary excretory function. • Hepatic uptake, storage, conjugation and excretion of bilirubin are finely balanced. Therefore, enhancement of bilirubin throughput requires coordinated induction of multiple genes, which may be mediated by nuclear receptors.
Sources of bilirubin Erythroid Non-erythroid (80%) (20%) • Normal: • Senescent erythrocytes Free heme • Abnormal: • Hemolysis:Extravascular Intravascular • Ineffective erythropoiesis • Cytochromes • Catalase • Peroxidase • Tryptophane pyrrolase • Myoglobin
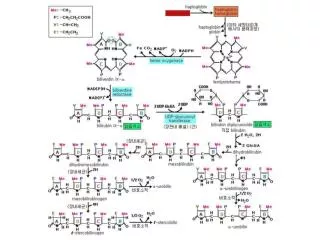
Opening of the heme ring and Enzyme-catalyzed formation of bilirubin
OH O CH2 V M M CH2 N N CH2 H H O The linear structure of bilirubin: Two dipyrroles joined by a central methene bridge O OH C C CH2 V M M CH2 N N H O H
Bilirubin contains several polar groups (shown in red): Yet, it is insoluble in water. O OH OH O C C CH2 CH2 V V M M M M CH2 CH2 N N N N CH2 H H O H O H
Conjugation with glucuronic acid makes bilirubin water soluble
The internal hydrogen bonds of bilirubin are disrupted by conjugation of the propionic acid carboxyl group with glucuronic acid CH2 C V M OH M CH2 O H H O N N N N CH2 H H O OH CH2 M M O CH2 V C
The internal hydrogen bonds of bilirubin are disrupted by conjugation of the propionic acid carboxyl group with glucuronic acid CH2 -GlucA C O V M M CH2 H H O N N N N CH2 H H O CH2 M M CH2 V GlucA- C O
Phototherapy changes the configuration of bilirubin makingit transiently water soluble
Tight junction Liver sinusoid Sinusoidal surface Fenestrated endothelium Canalicular surface Bilirubin throughput: schema of a hepatocyte
Bilirubin circulates bound to serum albumin. Albumin- binding: • Keeps bilirubin soluble • Prevents tissue deposi- tion. • Prevents renal excretion • Drugs that displace bilirubin from albumin may precipitate kernicterus: Sulfonamides Coumadin, etc. alb B
Bilirubin circulates bound to serum albumin. alb B • At the sinusoidal surface of hepatocytes, it dissociates from albumin.
Bilirubin circulates bound to serum albumin. alb B • At the sinusoidal surface of hepatocytes, it dissociates from albumin.
Bilirubin circulates bound to serum albumin. alb • At the sinusoidal surface of hepatocytes, it dissociates from albumin. B
Bilirubin circulates bound to serum albumin. alb • At the sinusoidal surface of hepatocytes, it dissociates from albumin. B
Bilirubin enters through the sinusoidal surface, probably by facilitated diffusion. Bilirubin uptakeis reduced: • In neonates • In cirrhosis • From drug effect: novobiocin • In some cases of Gilbert syndrome • Uptake is energy independent and bidirectional. B B
What is the mechanism of facilitated diffusion of bilirubin? • Zucker has proposed that no transporter protein is needed. • In a recent report, organic anion transport protein 2 (oatp2) has been implicated in bilirubin uptake. • However, oatp2 transports organic anions, such as BSP, it is not sufficient for bilirubin transport.
Inside the hepatocyte, bilirubin binds to cytosolic proteins termed ligandins, which are the same as glutathione-S- transferases (GSTs). GSTs GST bindinginhibits theefflux of bilirubin,thereby increasingits net uptake B B
GSTs B B
GSTs GA B • Conjugation of bilirubin with glucuronic acid is catalyzed by UGT1A1, which transfers glucuronic acid from UDP-glucuronic acid to bilirubin • Conjugation with glucuronic acid makes bilirubin water-soluble and non-toxic. • Glucuronidation is essential for biliary excretion of bilirubin. UDP UDPGA B B UGT1A1
UDP-glucuronosyltransferases (UGTs) UDPGA UDP • UGTs are ER proteins that convert many internal and exogenous toxins to non-toxic metabolites. • UGT’s are a family of enzymes concentrated in the liver. • One UGT isoform, UGT1A1, conjugates bilirubin and is essential for its excretion. • Inherited UGT1A1 deficiency causes jaundice. Substrate Glucuronide • UGT
Jaundice: • It is a medical term describes the elevation of bilirubin in blood result in yellow color of skin and sclera. • Other symptoms include nausea, vomiting, dark-colored urine and Types of Jaundice: • fatigue. • according to the cause of jaundice it is classified to three main types: • Pre-hepatic jaundice • Hepatic jaundice • Post-hepatic (most common type)
hemolytic jaundice hepatocellular jaundice obstructive jaundice
Thank you for your attention!