Download
1 / 16
200 likes | 1.07k Views
Jaundice. Tad Kim, M.D. UF Surgery tad.kim@surgery.ufl.edu (c) 682-3793; (p) 413-3222. Overview. Normal Physiology Pathophysiology Broad Differential Diagnosis DDx of Obstructive Jaundice Work-up for “Medical” Jaundice Work-up if Obstructive Jaundice Treatment of Obstructive Jaundice.

E N D
Jaundice Tad Kim, M.D. UF Surgery tad.kim@surgery.ufl.edu (c) 682-3793; (p) 413-3222
Overview • Normal Physiology • Pathophysiology • Broad Differential Diagnosis • DDx of Obstructive Jaundice • Work-up for “Medical” Jaundice • Work-up if Obstructive Jaundice • Treatment of Obstructive Jaundice
Normal Physiology • Bilirubin is from breakdown of hemoglobin • Unconjugated bilirubin transported to liver • Bound to albumin because insoluble in water • Transported into hepatocyte & conjugated • With glucuronic acid → now water soluble • Secreted into bile • In ileum & colon, converted to urobilinogen • 10-20% reabsorbed into portal circulation and re-excreted into bile or into urine by kidneys
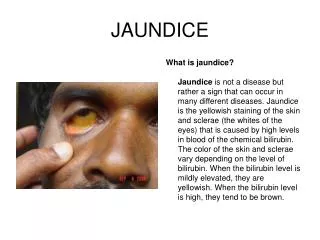
Pathophysiology • Jaundice = bilirubin staining of tissue @ lvl greater than ~2 • Mechanisms: • ↑ production of bilirubin • ↓ hepatocyte transport or conjugation • Impaired excretion of bilirubin • Impaired delivery of bilirubin into intestine • “surgically relevant jaundice” or obstructive jaundice • “Cholestasis” refers to the latter two, impaired excretion and obstructive jaundice
DDx: Unconjugated bilirubinemia • ↑production • Extravascular hemolysis • Extravasation of blood into tissues • Intravascular hemolysis • Errors in production of red blood cells • Impaired hepatic bilirubin uptake(trnsport) • CHF • Portosystemic shunts • Drug inhibition: rifampin, probenecid
DDx: Unconjugated bilirubinemia • Impaired bilirubin conjugation • Gilbert’s disease • Crigler-Najarr syndrome • Neonatal jaundice (this is physiologic) • Hyperthyroidism • Estrogens • Liver diseases • chronic hepatitis, cirrhosis, Wilson’s disease
DDx: Conjugated Bilirubinemia • Intrahepatic cholestasis/impaired excretion • Hepatitis (viral, alcoholic, and non-alcoholic) • Any cause of hepatocellular injury • Primary biliary cirrhosis or end-stage liver dz • Sepsis and hypoperfusion states • TPN • Pregnancy • Infiltrative dz: TB, amyloid, sarcoid, lymphoma • Drugs/toxins i.e. chlorpromazine, arsenic • Post-op patient or post-organ transplantation • Hepatic crisis in sickle cell disease
DDx: Obstructive Jaundice • This is the slide to remember for surgeons • Obstructive Jaundice– extrahepatic cholestasis • Choledocholithiasis (CBD or CHD stone) • Cancer (peri-ampullary or cholangioCA) • Strictures after invasive procedures • Acute and chronic pancreatitis • Primary sclerosing cholangitis (PSC) • Parasitic infections • Ascaris lumbricoides, liver flukes • Just remember top 5 (not parasites)
Initial Evaluation: History • Jaundice, acholic stools, tea-colored urine • Fever/chills, RUQ pain (cholangitis) • Could lead to life-threatening septic shock • Reasons to have hepatitis or cirrhosis? • Alcohol, Viral, risk factors for viral hepatitis • Exposure to toxins or offending drugs • Inherited disorders or hemolytic conditions • Recent blood transfusions or blood loss? • Is patient septic or on TPN? • Recent gallbladder surgery? (CBD injury)
Initial Evaluation: Physical Exam • Signs of end stage liver disease (cirrhosis) • Ascites, splenomegaly, spider angiomata, and gynecomastia • Jaundice evident first underneath the tongue, also evident in sclerae or skin • Courvoisier’s sign = painless, but palpable or distended gallbladder on exam • Could indicate malignant obstruction
Screening Labs • NL LFT r/o hepatic injury or biliary tract dz • Consider inherited disorders or hemolysis • ↑Alk Phos moreso than AST/ALT implies “cholestasis” (intrahepatic vs obstruction) • ↑Alk Phos also seen in sarcoid, TB, bone • In this case, GGT is specific for biliary origin • Predominant ↑AST/ALT implies intrinsic hepatocellular disease • AST/ALT ratio > 2 in alcoholic hepatitis • ↓albumin or ↑INR c/w advanced liver dz
Subsequent Labs • If no concern for obstructive jaundice: • Viral (Hep B&C) serologies for viral hepatitis • anti-mitochondrial Ab (PBC) • anti-smooth muscle Ab (Auto-immune) • iron studies (hemochromatosis) • ceruloplasmin (Wilson’s) • Alpha-1 anti-trypsin activity (for deficiency)
Imaging for Obstructive Jaundice • RUQ Ultrasound • See stones, CBD diameter • CT scan • Identify both type & level of obstruction • ERCP • Direct visualization of biliary tree/panc ducts • Procedure of choice for choledocholithiasis • Diagnostic –AND- therapeutic (unlike MRCP) • PTC useul of obstruction is prox to CHD • Endoscopic Ultrasound or EUS
Treatment • If Medical, then treat the etiology • If Obstructive Jaundice: • Should r/o ascending cholangitis, ABC/resusc • For cholangitis: IVF, IV Antibiotics, Decompression • Stones (remove stones vs stent vs drainage) • Done via ERCP or PTC or open (surgery) • Benign stricture (stent vs drainage catheter) • Cancer (Stent vs drainage +/- resect the CA) • The key principle is decompression, either externally(drainage) or internally(stenting) the duct open to allow better drainage
Take Home Points • Above is a comprehensive approach • For surgery clerkship, all you need to know is: • 1. Broad categories (no specific diagnoses) • 2. The four DDx of obstructive jaundice • 3. H&P (ask about fevers/chills, jaundice, acholic stools, dark urine, weight loss for CA), r/o ascending cholangitis = emergency • 4. Labs (LFT: ?cholestatic, CBC w diff, BMP) • 5. Imaging (U/S, CT, MRCP, EUS) • 6. Therapy (ERCP vs PTC vs surgery)