Download

1 / 15

E N D
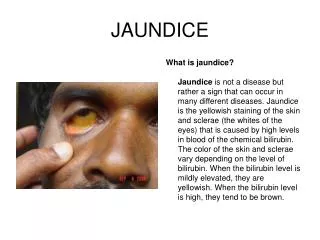
Approach to the Jaundiced Infant • Jaundice is present during the first week of life in 60% of term infants and 80% of preterm infants. There is usually an accumulation of unconjugated bilirubin, but there may also be deposition of direct bilirubin. During fetal life, the placenta is the principal route of elimination of unconjugated bilirubin. In the newborn infant, bilirubin is conjugated through the activity of glucuronyltransferase. In the conjugated form, bilirubin is water soluble, which results in its excretion into the biliary system and then into the GI tract. Newborns have a relatively high level of circulating hemoglobin and relative immaturity of the conjugating machinery. This results in a transient accumulation of bilirubin in the tissues, which is manifested as jaundice. Physiologic jaundice is evident by the second or third day of life and usually resolves within approximately 5 to 7 days. By definition, jaundice that persists beyond 2 weeks is considered pathologic.
Pathologic jaundice may be due to biliary obstruction, increased hemoglobin load, or liver dysfunction. The work-up of the jaundiced infant therefore should include a search for the following possibilities: (a) obstructive disorders, including biliary atresia, choledochal cyst, and inspissated bile syndrome; (b) hematologic disorders, including ABO incompatibility, Rh incompatibility, and spherocytosis; (c) metabolic disorders, including alpha1-antitrypsin deficiency, galactosemia, and pyruvate kinase deficiency; and (d) congenital infection, including syphilis and rubella.
Pathogenesis • Biliary atresia is a rare disease associated with significant morbidity and mortality. This disease is characterized by a fibroproliferative obliteration of the biliary tree that progresses toward hepatic fibrosis, cirrhosis, and end-stage liver failure. The incidence of this disease is approximately 1 in 5000 to 1 in 12,000. The etiology of biliary atresia is likely multifactorial. In the classic textbook Abdominal Surgery of Infancy and Childhood, Ladd and Gross described the cause of biliary atresia as an "arrest of development during the solid stage of bile duct formation." Previously proposed theories of the cause of biliary atresia have focused on defects in hepatogenesis, prenatal vasculogenesis, immune dysregulation, infectious agents, and exposure to toxins. More recently, genetic mutations in the cfc1 gene, implicated in left-right axis determinations, were identified in patients with biliary atresia–splenic malformation syndrome. In addition, the finding of a higher incidence of maternal microchimerism in the livers of males with biliary atresia has led to the suggestion that consequent expression of maternal antigens may lead to an autoimmune process that results in inflammation and obliteration of the biliary tree. Recent animal studies strongly implicate perinatal exposure to reovirus or rotavirus. Such viral exposure may lead to periportal inflammation mediated by interferon- and other cytokines.
Clinical Presentation • Infants with biliary atresia present with jaundice at birth or shortly thereafter. The diagnosis of biliary atresia is frequently not entertained by pediatricians, in part because physiologic jaundice of the newborn is so common and biliary atresia is so uncommon. For this reason, a delay in diagnosis is not unusual. However, infants with biliary atresia characteristically have acholic, pale gray stools, secondary to obstructed bile flow. With further passage of time, these infants manifest progressive failure to thrive and, if untreated, develop stigmata of liver failure and portal hypertension, particularly splenomegaly and esophageal varices.
The obliterative process of biliary atresia involves the common duct, cystic duct, one or both hepatic ducts, and the gallbladder, in a variety of combinations. Histopathologic findings for patients with biliary atresia include inflammatory changes in the parenchyma of the liver as well as fibrous deposition at the portal plates observed on trichrome staining of frozen tissue sections. In certain cases, bile duct proliferation may be seen, a relatively nonspecific marker of liver injury. Approximately 25% of patients with biliary atresia have coincidental malformations that are often associated with polysplenia and may include intestinal malrotation, preduodenal portal vein, and intrahepatic vena cava.
Diagnosis • In general, the diagnosis of biliary atresia is made using a combination of studies, because no single test is sufficiently sensitive or specific. Fractionation of the serum bilirubin is performed to determine if the associated hyperbilirubinemia is conjugated or unconjugated. Work-up commonly includes the analysis of TORCH (toxoplasmosis, other infections, rubella, cytomegalovirus infection, and herpes simplex) infection titers as well as tests for viral hepatitis. Typically ultrasonography is performed to assess for the presence of other causes of biliary tract obstruction, including choledochal cyst. The absence of a gallbladder is highly suggestive of the diagnosis of biliary atresia. However, the presence of a gallbladder does not exclude the diagnosis of biliary atresia, because in approximately 10% of biliary atresia patients, the distal biliary tract is patent and a gallbladder may be visualized, even though the proximal ducts are atretic. One should note that the intrahepatic bile ducts are never dilated in patients with biliary atresia.
In many centers, a nuclear medicine scan using technetium TC 99m disofenin, performed after pretreatment of the patient with phenobarbital, has proven to be an accurate and reliable study. If radionuclide appears in the intestine, the biliary tree is patent and the diagnosis of biliary atresia is excluded. If radionuclide is concentrated by the liver but is not excreted despite treatment with phenobarbital, and results of the metabolic screen, particularly alpha1-antitrypsin level, are normal, the presumptive diagnosis is biliary atresia. Percutaneous liver biopsy findings might potentially distinguish between biliary atresia and other sources of jaundice such as neonatal hepatitis. When the results of these tests point to or cannot exclude the diagnosis of biliary atresia, surgical exploration is warranted. At surgery, a cholangiogram may be performed if possible, using the gallbladder as a point of access. This may be accomplished using a laparoscope. The cholangiogram demonstrates the anatomy of the biliary tree, reveals whether extrahepatic bile duct atresia is present, and indicates whether there is distal bile flow into the duodenum. The cholangiogram may demonstrate hypoplasia of the extrahepatic biliary system. This condition is associated with hepatic parenchymal disorders that cause severe intrahepatic cholestasis, including alpha1-antitrypsin deficiency and biliary hypoplasia (Alagille syndrome). Alternatively, a cursory assessment of the extrahepatic biliary tree may clearly delineate the atresia.
Inspissated Bile Syndrome • The term inspissated bile syndrome is applied to patients with normal biliary tracts who have persistent obstructive jaundice. Increased viscosity of bile and obstruction of the canaliculi are implicated as causes. The condition has been seen in infants receiving parenteral nutrition, but it is also encountered in patients with disorders associated with hemolysis and in patients with cystic fibrosis. In some instances, no etiologic factors can be defined. Cholangiography is both diagnostic and therapeutic in inspissated bile syndrome.
Neonatal Hepatitis • Neonatal hepatitis may present in a similar fashion to biliary atresia. This disease is characterized by persistent jaundice due to acquired biliary inflammation without obliteration of the bile ducts. There may be a viral cause. The disease is usually self-limited.
Treatment • If the diagnosis of biliary atresia is confirmed intraoperatively, then surgical treatment is undertaken during the same procedure. Currently, first-line therapy consists of creation of a hepatoportoenterostomy, as described by Kasai. The purpose of this procedure is to promote bile flow into the intestine. • Some authors believe that an intussuscepted antireflux valve is useful in preventing retrograde bile reflux, although the data suggest that it does not influence outcome. A liver biopsy is performed at the time of surgery to determine the degree of hepatic fibrosis that is present. The diameter of bile ducts at the portal plate is predictive of the likelihood of long-term success of biliary drainage through the portoenterostomy. Numerous studies also suggest that the likelihood of surgical success is inversely related to the age at the time of portoenterostomy. Infants treated before 60 days of age are more likely to achieve successful and long-term biliary drainage than are older infants. Although the outlook is less favorable for patients after the twelfth week, it is reasonable to proceed with surgery even beyond this point, because the alternative is certain liver failure. It is noteworthy that a significant number of patients have had favorable outcomes after undergoing portoenterostomy despite advanced age at the time of diagnosis.
Bile drainage is anticipated when the operation is carried out early; however, bile flow does not necessarily imply cure. Approximately one third of patients remain symptom free after portoenterostomy; the remainder require liver transplantation due to progressive liver failure. Independent risk factors that predict failure of the procedure include bridging liver fibrosis at the time of surgery and postoperative cholangitic episodes. A recent review of the data of the Japanese Biliary Atresia Registry, which includes the results for 1381 patients, showed that the 10-year survival rate was 53% without transplantation and 66.7% with transplantation. A common postoperative complication is cholangitis. There is no effective strategy to completely eliminate this complication, and the effectiveness of long-term prophylactic antibiotics has not been fully resolved.