Download
1 / 36
410 likes | 708 Views
Tolerance, autoimmunity and the pathogenesis of immune-mediated inflammatory diseases Abul K. Abbas UCSF. Balancing lymphocyte activation and control. Activation Effector T cells. Tolerance Regulatory T cells. Normal: reactions against pathogens Inflammatory

E N D
Tolerance, autoimmunity and the pathogenesis of immune-mediated inflammatory diseases Abul K. Abbas UCSF
Balancing lymphocyte activation and control Activation Effector T cells Tolerance Regulatory T cells Normal: reactions against pathogens Inflammatory disease, e.g. reactions against self No response to self Controlled response to pathogens
The importance of immune regulation • To avoid excessive lymphocyte activation and tissue damage during normal protective responses against infections • To prevent inappropriate reactions against self antigens (“self-tolerance”) • Failure of control mechanisms is the underlying cause of immune-mediated inflammatory diseases
General principles of controlling immune responses • Responses against pathogens decline as the infection is eliminated • Apoptosis of lymphocytes that lose their survival signals (antigen, etc) • Memory cells are the survivors • Active control mechanisms may function to limit responses to persistent antigens (self antigens, possibly tumors and some chronic infections) • Often grouped under “tolerance”
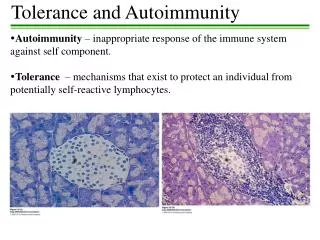
Immunological tolerance • Definition: • specific unresponsiveness to an antigen that is induced by exposure of lymphocytes to that antigen (tolerogen vs immunogen) • Significance: • All individuals are tolerant of their own antigens (self-tolerance); breakdown of self-tolerance results in autoimmunity • Therapeutic potential: Inducing tolerance may be exploited to prevent graft rejection, treat autoimmune and allergic diseases, and prevent immune responses in gene therapy
Autoimmunity • Definition: immune response against self (auto-) antigen, by implication pathologic • Disorders are often classified under “immune-mediated inflammatory diseases” • General principles: • Pathogenesis: Susceptibility genes + environmental triggers • Systemic or organ-specific
Central and peripheral tolerance The principal fate of lymphocytes that recognize self antigens in the generative organs is death (deletion), BUT: Some B cells may change their specificity (called “receptor editing”) Some CD4 T cells may differentiate into regulatory (suppressive) T lymphocytes From Abbas, Lichtman and Pillai. Cellular and Molecular Immunology 6th ed, 2007
Consequences of self antigen recognition in thymus From: Abbas & Lichtman, Cellular & Molecular Immunology 5th ed 2003
Central tolerance • Lymphocytes that see self antigens before they are mature are either eliminated or rendered harmless • Probably continues to occur at some level throughout life (as new lymphocytes are produced from bone marrow stem cells) • Role of the AIRE protein in thymic expression of some tissue antigens
APC APC APC APC Peripheral tolerance T cell CD28 Normal T cell response Activated T cells TCR Functional unresponsiveness Anergy Off signals TCR Activated T cell Apoptosis (activation-induced cell death) Deletion Block in activation Suppression Regulatory T cell
T cell anergy • Multiple mechanisms demonstrated in different experimental systems • No clear evidence that natural self antigens induce T cell anergy (especially in humans) • Therapeutic potential: can we administer antigens in ways that induce T-cell anergy?
“Activation-induced cell death”: death of mature T cells upon recognition of self antigens From Abbas and Lichtman. Basic Immunology 2nd ed, 2006 Both pathways cooperate to prevent reactions against self
Regulatory T cells From Abbas, Lichtman and Pillai. Cellular and Molecular Immunology 6th ed, 2007
Properties of regulatory T cells • Phenotype: CD4, high IL-2 receptor (CD25), low IL-7 receptor, Foxp3 transcription factor; other markers • Mechanisms of action: multiple • secretion of immune-suppressive cytokines (TGF, IL-10, IL-35), • inactivation of dendritic cells or responding lymphocytes
Thymic (“natural”) regulatory T cells (Treg) • Development requires recognition of self antigen during T cell maturation • Reside in peripheral tissues to prevent harmful reactions against self
Peripheral (adaptive, inducible) regulatory T cells • Develop from mature CD4 T cells that are exposed to persistent antigen in the periphery; no role for thymus • May be generated in all immune responses, to limit collateral damage • Can be induced in vitro (stimulation of CD4 T-cells in presence of TGF + IL-2) • What factors determine the balance of effector cells and Treg?
Signals for the generation and maintenance of regulatory T cells • Antigen recognition, with or without inflammation? • TGF- (source?) • Interleukin-2 (originally identified as T cell growth factor; major function is to control immune responses by maintaining functional Treg; works via Stat5) • Low levels of B7: CD28 costimulation • Transcription factor Foxp3 • Many activated T cells (not only Treg) may transiently express Foxp3
Regulatory T cells • Explosion of information about the generation, properties, functions and significance of these cells • Some autoimmune diseases are associated with defective generation or function of Tregs or resistance of effector cells to suppression by Tregs • Will cellular therapy with ex vivo expanded Treg become a reality? • Therapeutic goal: selective induction or activation of Treg in immune diseases
Immune-mediated inflammatory diseases • Chronic diseases with prominent inflammation, often caused by failure of tolerance or regulation • RA, IBD, MS, psoriasis, many others • Affect 2-5% of people, incidence increasing • May result from immune responses against self antigens (autoimmunity) or microbial antigens (Crohn’s disease?) • May be caused by T cells and antibodies • May be systemic or organ-specific
Features of autoimmune diseases • Fundamental problem: imbalance between immune activation and control • Underlying causative factors: susceptibility genes + environmental influences • Immune response is inappropriately directed or controlled; effector mechanisms of injury are the same as in normal responses to microbes • Nature of disease is determined by the type of dominant immune response • Many immunological diseases are chronic and self-perpetuating
Pathogenesis of autoimmunity Environmental trigger (e.g. infections, tissue injury) Susceptibility genes Failure of self-tolerance Activation of self-reactive lymphocytes Persistence of functional self-reactive lymphocytes Immune responses against self tissues
Genetics of autoimmunity • Human autoimmune diseases are complex polygenic traits • Identified by genome-wide association mapping • Single gene mutations are useful for pathway analysis • Some polymorphisms are associated with multiple diseases • May control general mechanisms of tolerance and immune regulation • Other genetic associations are disease-specific • May influence end-organ damage
Genetics of autoimmunity: recent successes of genomics • NOD2: polymorphism associated with ~25% of Crohn’s disease • Microbial sensor • PTPN22: commonest autoimmunity-associated gene; polymorphism in RA, SLE, others • Phosphatase • CD25 (IL-2R): associated with MS, others; genome-wide association mapping • Role in Tregs
Infections and autoimmunity • Infections trigger autoimmune reactions • Clinical prodromes, animal models • Autoimmunity develops after infection is eradicated (i.e. the autoimmune disease is precipitated by infection but is not directly caused by the infection) • Some autoimmune diseases are prevented by infections (type 1 diabetes, multiple sclerosis, others? -- increasing incidence in developed countries): mechanism unknown • The “hygiene hypothesis”
Immune-mediated diseases • The nature of the disease is determined by the type of dominant immune response • Th1 response: inflammation, autoantibody production; autoimmune diseases • Th2 response: IgE+eosinophil-mediated inflammation; allergic reactions • Th17 response: acute (and chronic?) inflammation; increasingly recognized in immune-mediated diseases
CD4 T cell subsets: function Th1 cells (IFN-g) Host defense: many microbes Systemic and organ-specific autoimmune diseases Th2 cells (IL-4, IL-5) Host defense: helminths Allergic diseases Naïve CD4 T cell Th17 cells (IL-17) Host defense: fungi, bacteria Organ-specific autoimmune diseases Regulatory T cells
CD4 subsets: generation and function Th1 cells (IFN-g) Host defense: many microbes Systemic and organ-specific autoimmune diseases Th2 cells (IL-4, IL-5) IFN-, IL-12: T-bet, Stat4 Host defense: helminths Allergic diseases IL-4: GATA3, Stat6 Naïve CD4 T cell Th17 cells (IL-17) TGF- + IL-6:RORt, Stat3 TGF-IL-2: Foxp3, Stat5 Host defense: fungi, bacteria Organ-specific autoimmune diseases Regulatory T cells
Subsets of CD4+ T cells • Dominant T cell subsets determine disease vs protection • Many autoimmune and allergic diseases are associated with imbalance of T cell subsets • Cytokines and transcription factors involved in differentiation of naïve T cells to different subsets are well defined, especially in vitro • Conditions for induction in vivo? in disease? • Stability or plasticity of subsets?
Immune-mediated diseases • Immunological diseases tend to be chronic and self-perpetuating, because -- • The initiating trigger can often not be eliminated (self antigen, commensal microbes) • The immune system contains many built-in amplification mechanisms whose normal function is to optimize our ability to combat infections • “Epitope spreading”
Amplification loop in cell-mediated immunity Cytokines are powerful amplifiers of immune reactions
Pathogenesis of organ-specific autoimmunity Current therapies target late stages of the reaction (lymphocyte activation, inflammation). Ultimate goal should be to tackle the underlying cause and restore control of the abnormally directed response
Immune-mediated inflammatory diseases • Immune-mediated inflammatory diseases develop because the normal controls on immune responses fail • The phenotype of the disease is determined by the nature of the immune response • These diseases often become self-perpetuating
Animal models of human inflammatory diseases: how good are they? • Resemblance to human diseases: • Same target organs involved • Often similar effector mechanisms (antibodies, cytokines, cytotoxic T lymphocytes) • Differences from human diseases: • Unknown underlying susceptibility genes (some similarities, e.g. in type 1 diabetes) • Often induced by experimental manipulation, e.g. overt immunization with tissue antigen, inflammatory stimulus, or transgenic approach • The potential of “humanized” mice?
Biomarkers of human immune diseases • Major goal of current research • High-throughput screens for transcripts and proteins associated with disease • Many practical limitations: • Reliance on population assays, even though only a small fraction of total lymphocytes may be abnormal in control/activation • Use of blood cells, even though the relevant reactions may be in tissues • Nevertheless, emerging successes: • Type I interferon “signature” in lupus
Immune-mediated inflammatory diseases • Experimental models are revealing pathways of immune regulation and why it fails • Genetic studies are identifying underlying defects in human diseases • Improving technologies are enabling analyses of patients • Challenges: • From genes to pathways (molecular and functional) • Using the knowledge to develop therapies