Download
1 / 32
460 likes | 1.27k Views
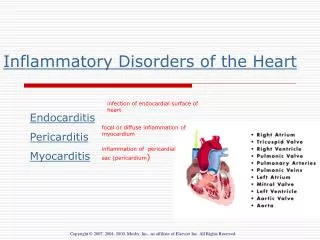
Inflammatory Diseases of the Heart. Objectives. Describe inflammatory disorders of the cardiovascular system Explain the pathophysiology of common inflammatory disorders Describe nursing interventions in caring for clients with inflammatory disorders. Rheumatic Heart Disease.

E N D
Objectives • Describe inflammatory disorders of the cardiovascular system • Explain the pathophysiology of common inflammatory disorders • Describe nursing interventions in caring for clients with inflammatory disorders
Rheumatic Heart Disease • Rheumatic Fever develops after an infection caused by group A beta-hemolytic streptococcal pharyngitis
Rheumatic Heart Disease • Inflammation of endocardium, myocardium, and/or pericardium develops small areas of necrosis which when healed, leave scar tissue • Damage to the endocardium will later cause valve disease nodules that become fibrous and incompetent. With healing, valves become thick and deformed stenosis and insufficiency development of heart murmur
Rheumatic Heart Disease • Treatment: PCN or –mycins, anti-inflammatory drugs
Endocarditis • Infective or bacterial endocarditis • An infection or inflammation of the inner membranous lining of the heart, esp. valves • Most common causes IV drug abuse, Rheumatic heart disease, prosthetic heart valves (within 60 days of surgery) • Also caused by dental procedures in vulnerable patients
Endocarditis • Infectious pathogen causes fibrin and platelets to aggregate on endocardium causing “vegetation” (friable and wart-like tissue) • Vegetation will cause ulceration and necrosis of tissue. Vegetations can also break off and embolize
Endocarditis • Diagnostic Tests • Positive blood cultures • Elevated WBC and ESR • Anemia • Positive Rheumatoid Factor • Echocardiogram • Electrocardiogram – a change will reveal HF and cardiomegaly
Endocarditis • Signs and Symptoms • Weight loss, anorexia • Malaise, fever, chills, night sweats, joint pain • Valve regurgitation/insufficiency (murmur)
Endocarditis • Splinter Hemorrhages: Short, thin, brown, linear streaks in the nails • Osler's nodes are painful, red, raised lesions on the fingers and sometimes seen on the soles of the feet. • Janesway lesions are non-tender, small erythematous or hemorrhagic macules or nodules in the palms or soles
Endocarditis Janesway lesions Osler’s Nodes Splinter Hemorrhages
Treatment of Endocarditis • PCN and usually Gentamycin • Rest – to ↓ workload • Bedrest if pt. has ↑ temp + s/sx HF • Rehydration • May require surgery for affected valves • If prosthetic valve is already in place it will need to be replaced
Endocarditis • Medical Goals: • Support cardiac function • Destruction of pathogen • Prevention of complications • ↑ risk emboli
Myocarditis • Inflammation of the myocardium caused by a pathogen – virus, fungi, bacteria • May also be caused by endocarditis or pericarditis • May lead to hypertrophy, fibrosis, and decreased contractility leading to dilation of the chambers and possibly damage the conduction system dysrrhytmias
Myocarditis Diagnostic Tests • X-ray shows enlarged heart • Elevated cardiac enzymes • Blood Cultures • Biopsy • EKG • Echocardiography
Myocarditis Signs and symptoms: • Fatigue, dyspnea, palpations • Mild to moderate, dull and continuous CP • Tachycardia • Mitral regurgitation-murmur • Pericardial friction rub • Heart failure
Treatment of Myocarditis • Antibiotics and Anti-inflammatory meds • Rest • Treatment of further complications: • Heart failure • Valvular insufficiency
Pericarditis • Inflammation of the pericardium – the sac that surrounds the heart • May be fibrous inflammation or collection of fluid • Fluid may be purulent, serous, or sanguineous • Caused by: • Damage from a pathogen and the immune response releasing inflammatory mediators • Malignancy
Pericarditis • Fibrous constriction and thickness compression around the heart severe enough to prevent normal filling during diastole • As the inflammatory process continues, more fluid builds up in the pericardial space • Chronic pericarditis is a stiff pericardium caused by the damage of acute pericarditis
Pericarditis • Diagnostic Tests • EKG shows diffuse ST Elevation • Elevated cardiac enzymes • Elevated WBC, ESR, CRP • Positive blood cultures • Echocardiogram and CXR
Pericarditis • Signs and symptoms • Sharp chest pain • Fever, chills • Muffled heart sounds, friction rub (grating, scratching) • Heart failure- decreased cardiac output, Jugular venous distension, dyspnea, shallow respirations
Constrictive Pericarditis • Often unable to differentiate between Restrictive CM and Constrictive Pericarditis • Biggest difference: Constrictive Pericarditis can be cured with pericardial stripping.
Constrictive Pericarditis • Constrictive pericarditis is due to: • A thickened, fibrotic pericardium that forms a non-compliant shell around the heart. • This shell prevents the heart from expanding when blood enters it. • Constrictive Pericarditis can be cured with pericardial stripping.
Treatment of Pericarditis • Antibiotics • Anti-inflammatory medications • Bedrest • Pain medication for CP • Pericardiocentesis
Cardiac Tamponade • Too much fluid in the pericardial sac compresses the heart and impairs systole and diastole • Fluid may accumulate slowly or suddenly • Cardiac Output is significantly decreased • Patient will rapidly decline
Cardiac Tamponade • Diagnostic Tests • CXR widened mediastinum and enlarged heart • Echocardiogram shows pericardial effusion • Signs and Symptoms • Muffled heart sounds, s/s of low cardiac output, cyanosis • Restlessness, anxiety, impending doom • JVD • Tachycardia • Cough, SOB, Tachypnea, orthopnea
Cardiac Tamponade • Narrowed pulse pressure (SBP-DBP) • Beck’s Triad • Pulsus paradoxus • Muffled heart sounds • JVD • Pulsus Paradoxus • SBP decreases on inspiration
Nursing Implications • Goals - Treating S&S - Treating & preventing further infection - Minimizing cardiac demands - Comfort