Download
1 / 27
270 likes | 860 Views
Infections of the genitourinary system. Incidental Nosocomial Sexually transmitted. Anatomy of the urinary system. Kidneys filter blood Ureters carry urine to bladder Bladder stores urine until it is expelled (through urethra) Protected from infection by anatomy and function.

E N D
Infections of the genitourinary system Incidental Nosocomial Sexually transmitted
Anatomy of the urinary system • Kidneys filter blood • Ureters carry urine to bladder • Bladder stores urine until it is expelled (through urethra) • Protected from infection by anatomy and function
Male and female genital systems • Close proximity to urinary system contributes to risk of infection • Portal of entry for many pathogens • Genital system has several possible sites for establishing infections
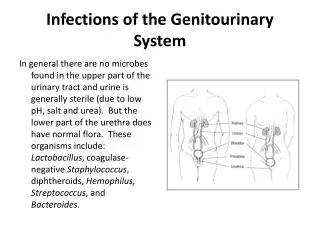
Normal flora • Urinary system • Generally confined to urethra • Lactobacilli, Gram-positive cocci, Haemophilus • Genital system • Females: can vary depending on hormonal activity (estrogen indirectly promotes acid pH) • Vaginal infections more common in girls and postmenopausal women • Males: normal flora in urethra below prostate • Lactobacilli, Staphylococci, streptococci
Urinary tract infections (UTIs) • Major cause of nosocomial infections (interference with normal urinary function) • Common infections in general • More in males than females • Anatomy; poor hygiene usually the cause • Restriction of urine flow can contribute to incidence of infection • Can enter urinary system from other organ systems
Cystitis (bladder infections) • Usually due to E. coli; also Proteus, Klebsiella, Staphylococcus • In hospitals, acquired through catheters • Bacteria have pili that enable attachment • Much more common in women • Pyelonephritis is a serious possible consequence • Treatment: hydration and antibiotics
Leptospirosis • Common zoonosis • Enters body through bloodstream • Can survive outside the body for weeks • Try to avoid animal urine
Genital infections that are not sexually transmitted (non-venereal) • Vaginosis associated with smelly discharge • pH in vagina is elevated (anything above 4.5 is considered high) • Normal flora of vagina is disrupted • Gardnerella vaginalis and various anaerobes are implicated • Is it sexually transmitted?
Significance of vaginosis • Linked to premature or low-birthweight deliveries • Linked to pelvic inflammatory disease (PID) • Linked to increased susceptibility to AIDS • Metronidazole (cream) is treatment of choice
Vaginosis vs. candidiasis vaginosis • Both signify disruption of normal flora • Neither is thought to be a STD • One is fungal, one bacterial • Candidiasis may arise after antibiotic treatment, use of oral contraceptives, diabetes
Bacterial STDs: gonorrhea (Neisseria gonorrhoeae) • Lives on mucous membranes of humans • Transmitted by direct contact • Attach to non-ciliated cells; form pili • Antigenic variation: • Can attach to different types of cells • Can evade immune system • Can inhibit T-helper cells (Opa proteins)
Men: Asymptomatic or painful urination Scarring can impede urine flow Scarring of vas deferens or damage to testes can cause sterility Can infect urethra and other areas (cervix, uterine tubes, etc. ) PID moves into abdominal cavity Can lead to sterility Can infect eyes of fetus during birth Carrier state possible in both sexes No immunity in either sex Effects of untreated gonorrhea in men and women
Chlamydia: the most common infectious agent • Complications are much more likely in males than females • Half or more cases are asymptomatic • Can be transmitted nonsexually • Infected mother can transmit chlamydia to newborns (conjunctivitis, pneumonia) • Readily treated with antibiotics (azithromycin; tetracycline; erythromycin)
Syphilis: “the great imitator” • Primary syphilis: chancre about 3 weeks after infection • Secondary syphilis 2-10 weeks later: flu-like symptoms • Tertiary syphilis (years later): degeneration of the nervous system
Pathogenesis • Invades mucous membranes and skin lesions • Chancre SOMETIMES forms at site of infection and spontaneously disappears • Organisms evade killing by immubne system
Secondary syphilis • Mucous patches are highly infectious • (can be transmitted in saliva) • Stage can last up to one year • About 50% of cases do not progress past this stage Inside of mouth
Tertiary syphilis • Gummas can appear anywhere, even bones • Not infectious • Neurological damage usually seen around 20 years after initial infection
Diagnosing syphilis • Wassermann test (early 1900’s)- no cures, but could identify infected persons. Significance: first effective screening test for syphilis • Other antibody tests are faster, more specific and more accurate • Can identify Treponema bacteria in early stages; few bacteria present in tertiary stages
Treating syphilis • Can be treated with Penicillin G in early stages (azithromycin if allergic) • Tertiary stage is hyperimmune reaction and few bacteria are present- so does not respond well to antibiotics • Preventions- abstinence, monogamy, safe sex
Viral STDs are not curable Ulcer dries up within 2-3 weeks • Genital herpes simplex • Symptoms appear about 1 week after exposure • Blisters on exposed areas, which then ulcerate. Blisters shed virus, which can infect esophagus, eyes or skin (whitlow) • Whitlow can be caused by herpes simplex 1 or 2
Epidemiology, avoidance and treatment • Herpes simplex 2 is almost always sexually transmitted • Abstinence during outbreaks; condom use • Pregnant women with genital herpes should not give birth vaginally • Acyclovir can help control symptoms • No cure
Human papilloma virus • Many different types of virus • Cause warts in about half of infected people about 3-8 weeks after infection • Infects deep layers of epithelium • Precancerous lesions of cervix are usually asymptomatic • HPV vaccine is directed against four common viruses that cause genital warts and cancer
HIV/AIDS • In US, caused by retrovirus HIV-1 • Attacks T-helper cells (CD4+) and macrophages • Spread sexually, to newborns and through blood • Combinations of reverse transcriptase and protease inhibitors can control disease • Vaccine is not yet available • Prevention is best method of avoidance
Protozoans STDs • Trichomonas vaginalis • Worldwide distribution among humans • Often asymptomatic • Disease is probably inflammatory • Organism is actually pretty fragile- no cyst formation • Responds to metronidazole
Summary • Disease-causing organisms are many, varied and well-adapted to the urogenital system • Often asymptomatic, therefore diagnosis and treatment are often belated • Control of infection usually requires a behavioral component • Vaccine development is often problematic