Download
1 / 30
310 likes | 423 Views
Module 1 Introduction. Exercise Instructions. Goal : You have 1 minute to build the tallest tower. Roles: Runners and Builders Rules: Blocks are located at the front and back of the room. Runners retrieve blocks from bins but may only take 5 blocks at a time.

E N D
Exercise Instructions Goal: You have 1 minute to build the tallest tower. Roles: Runners and Builders Rules: • Blocks are located at the front and back of the room. • Runners retrieve blocks from bins but may only take 5 blocks at a time. • Builders build the tower using the pattern of 1 large, 3 small blocks, repeat. • No two blocks of the same color may touch. • Runners are not allowed to build/ builders are not allowed to run. • Any unused blocks that are not replaced in the storage bins before time is called will result in subtraction from the tower height; one block subtracted for each unused block. Report Out: Height of tower in blocks (minus unused blocks).
Exercise Instructions Debrief: • What went well? • What didn’t go well? • What will you do differently? • Same pattern we will follow in simulation • Plan (Brief), Do, Study (Debrief), Repeat
Objectives • Describe the impact of errors and why they occur • Describe the TeamSTEPPS framework • Describe the TeamSTEPPS training initiative • State the outcomes of the TeamSTEPPS framework
Sue Sheridan Video Videos must be saved in the same file as your power point before you can insert them. • Click on insert tab in power point • Click on Video • Click on Video from file • Click on Sue SheridanLg001 • Click on Insert
Video Discussion • Patients are harmed as a result ofpoor communication and teamwork that results in medical errors • How often do medical errors occur? • Why do medical errors occur? • How can we prevent medical errors? • Applies to non-clinical situations…goals are not achieved …Improved teamwork and communications… Ultimately, a culture of safety Are you ready to be part of the transformation of health care?
How Often do Medical Errors Occur? • 44,000 – 98,000 deaths per year in hospitals due to medical errors IOM (2000). To Err is Human: Building a Safer Health System • Equal to one jumbo jet crashing EVERY DAY! • Where is CNN? (Photo: Ezra Shaw, Getty Images) www.foxnews.com
Impact of Medical Errors • From a 2010 analysis of a claims database • 1.8% of hospital admissions experience a medical error (a preventable adverse outcome of medical care) • Medical errors cost the US at least $19.5 billion/year • From a random sample of 780 Medicare beneficiaries discharged Oct. 2008 • 13.5% of hospitalized Medicare beneficiaries experience an adverse event (44% were preventable) • 1.5% experienced an event that contributed to their deaths (projects to 15,000 total patients/month) http://www.soa.org/files/pdf/research-econ-measurement.pdf http://oig.hhs.gov/oei/reports/oei-06-09-00090.pdf
Human Factors • Study of the interaction between humans and elements of the system in which they live/work • Physical environment • Tasks • Tools/technology • Organizational conditions • Goal: achieve optimal interaction between social, technical, and physical elements of a system. https://www.hfes.org//Web/AboutHFES/about.html
Why Do Errors Occur—Some Human Factors • Excessive professional courtesy • Halo effect • Passenger syndrome • Rigid Hierarchies • High-risk phase • Strength of an idea • Task fixation (lack of situational awareness) • Workload fluctuations • Interruptions • Fatigue • Multi-tasking • Failure to follow up • Poor handoffs • Ineffective communication • Not following protocol • Complacency
Turn to your neighbor… Human Factors 1. Describe a human error that you made. I ran a stop light. Which human factors contribute to this error? 2. Describe a recent error made at your hospital. CNA had pt use IV pole to walk to bathroom; pt’s legs buckled and she fell. Walker & gait belt were in room. Which human factors contributed to this error?
Joint Commission Sentinel Events http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004_2Q2012.pdf 14
The Problem… “The problem is not bad people; the problem is that the system needs to be made safer . . .” “People make fewer errors when they who work in teams.” IOM (2000). To Err is Human: Building a Safer Health System
Teamwork Is All Around Us Common purpose Performance goals Mutual accountability Clear role expectations Complementary skills Interdependent tasks
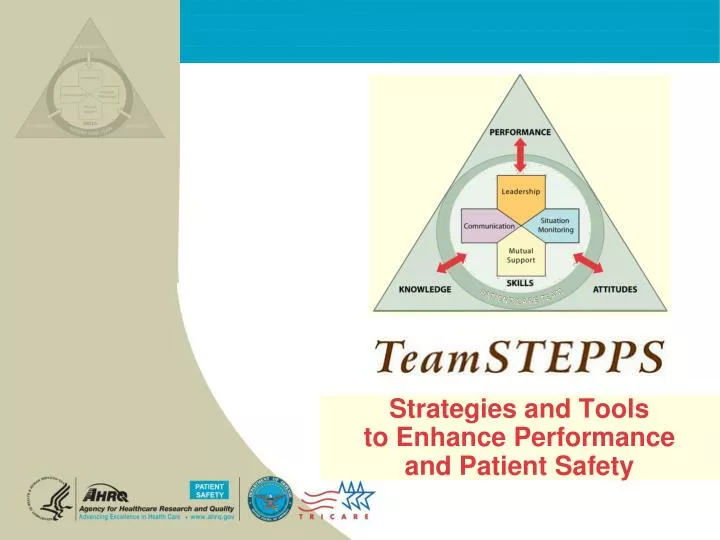
“Initiative based on evidence derived from team performance…leveraging more than 30 years of research in military, aviation, nuclear power, business and industry…to acquire team competencies” Team Strategies & Tools to Enhance Performance & Patient Safety
Evolution of TeamSTEPPS Curriculum Contributors • Department of Defense • Agency for Healthcare Research and Quality • Research Organizations • Universities • Medical and Business Schools • Healthcare Foundations • Hospitals—Military and Civilian, Teaching and Community-Based • Private Companies • Subject Matter Experts in Teamwork, Human Factors, and Crew Resource Management (CRM)
Evolution of TeamSTEPPS: US Army Aviation • Army aviation crew coordination failures in mid-80s contributed to 147 aviation fatalities and cost more than $290 million • The vast majority involved highly experienced aviators • Failures were largely attributedto crew communication, workload management, and task prioritization
Evolution of TeamSTEPPS: US Air Force CRM History • Mid to Late 80s AF bombers and heavy aircraft started CRM training • 1992 Air Combat Command developed Aircrew Attention Management /CRM Training • By 1998, CRM deployed uniformly across the AF • Steady decline in human factors based mishaps since CRM training deployed • AF Medical Service adapted training, rolled out in 2000
Mutual Performance Monitoring The Theory Team Leadership Team Orientation Back-up Behavior Shared Mental Models Mutual Trust Adaptability Team Effectiveness Big 5 Salas, Sims, Burke. Is there a “Big Five” in teamwork? Small Group Research. 2005; 36:555-599. Coord. Mechanism Closed Loop Communication
The Framework: What Comprises Team Effectiveness? KnowledgeCognitions“Think” AttitudesAffect“Feel” …team performance is a science…consequences of errors are great… SkillsBehaviors“Do”
More Evidence • Exploding Literature • Patient Care Team + Evidence-Based Practice = 1,128 • Patient Care Team + Evaluation Studies = 843 • Studies in diverse patient populations demonstrate relationship between teamwork and • Improved clinical processes • Reduction in medical errors • Improved surgical team performance • Increased adherence to guidelines • Decreased length of stay • Increased functional status • Decreased mortality Salas et al. What are the critical success factors for team training in health care? Jt Comm Jrnl Qual Safe. 2009;35:398-405.
Your Contribution to the Evidence • Team training can result in transformational change in safety culture when the work environment supports the transfer of learning to new behavior. • Hospital Survey on Patient Safety Culture conducted in 24 hospitals before training one year after training • To successfully implement and sustain new behaviors • Stay connected to the community via monthly calls • Train supervisors/managers first so they can role model behaviors • Provide multiple follow-up learning opportunities • Job descriptions/performance evaluations include use of team skills Jones KJ, Skinner AM, High R, Reiter-Palmon R. A theory-driven longitudinal evaluation of the impact of team training on safety culture in 24 hospitals. BMJ Qual Saf. 2013;22:394-404.
Supported by AHRQ 10 18 UNMC 5 58 1 Washington -TRC Minnesota -TRC North Shore Long I. TRC Duke TRC 1 Tulane TRC http://teamstepps.ahrq.gov/aboutnationalIP.htm
How Does TeamSTEPPS Work? Shift Towards a Culture of Safety
HSOPS Teamwork (Belief/Attitude) (Behavior) Practices/skills that bridge the gap • Identify team leaders • Set team goals • Use briefs, huddles, debriefs • Cross monitor (“watch each others’ back”) 32% GAP
DAY 1 Module 1—Introduction Module 2—Team Structure Module 3—Leadership Module 4—Situation Monitoring Module 5—Mutual Support Module 6—Communication Module 7—Summary—Putting It All Together DAY 2 Coaching Workshop High Fidelity Simulation Practice team skills Coach team skills Identify team skills Webinars to Complete Requirements for Master Trainer Certification Wed. Oct. 16 10 - 11 a.m. Thurs. Nov. 21 2 – 3 p.m. Agenda
TOOLS and STRATEGIES Brief Huddle Debrief Situational Monitoring Situational Awareness STEP Cross Monitoring Feedback Advocacy and Assertion Two-Challenge Rule CUS DESC Script Collaboration SBAR Call-Out Check-Back Handoff OUTCOMES • Shared Mental Model • Adaptability • Team Orientation • Mutual Trust • Team Performance • Patient Safety!! Training BARRIERS to Team Performance • Inconsistency in Team Membership • Lack of Time • Lack of Information Sharing • Hierarchy • Defensiveness • Conventional Thinking • Complacency • Varying Communication Styles • Conflict • Lack of Coordination and Follow-Up with Co-Workers • Distractions • Fatigue • Workload • Misinterpretation of Cues • Lack of Role Clarity
Summary • Impact of errors…patients are harmed, non-clinical teams do not achieve goals • TeamSTEPPS Framework • Safety net for fallible human beings • TeamSTEPPS training meets a need • Diffuse evidence-based training program nationally and internationally http://teamstepps.ahrq.gov/ • Outcomes of TeamSTEPPS Shared Mental Model Adaptability Team Orientation Mutual Trust Team Performance Patient Safety!!