Download
1 / 70
780 likes | 1.92k Views
Prepared by: June C Carroll MD CCFP FCFP Sydney G. Frankfort Chair in Family Medicine Associate Professor, Department of Family & Community Medicine Mount Sinai Hospital, University of Toronto Andrea L Rideout MS, CGC, CCGC Certified Genetic Counsellor

E N D
Prepared by: June C Carroll MD CCFP FCFP Sydney G. Frankfort Chair in Family Medicine Associate Professor, Department of Family & Community Medicine Mount Sinai Hospital, University of Toronto Andrea L Rideout MS, CGC, CCGC Certified Genetic Counsellor Project Manager – The Genetics Education Project Funded by: Ontario Women’s Health Council Version: February 2006 Comparison of Prenatal Screening Tests for the Detection of Down Syndrome
Acknowledgements Reviewed by: Members of The Genetics Education Project Committee Funded by: The Ontario Women's Health Council as part of its funding to The Genetics Education Project * Health care providers must use their own clinical judgment in addition to the information presented herein. The authors assume no responsibility or liability resulting from the use of information in this presentation.
Outline • Prenatal screening options for chromosome disorders -current and new technologies • Women’s information needs • to facilitate informed choice • Case examples • What’s on the horizon in prenatal genetic screening? • Bottom line
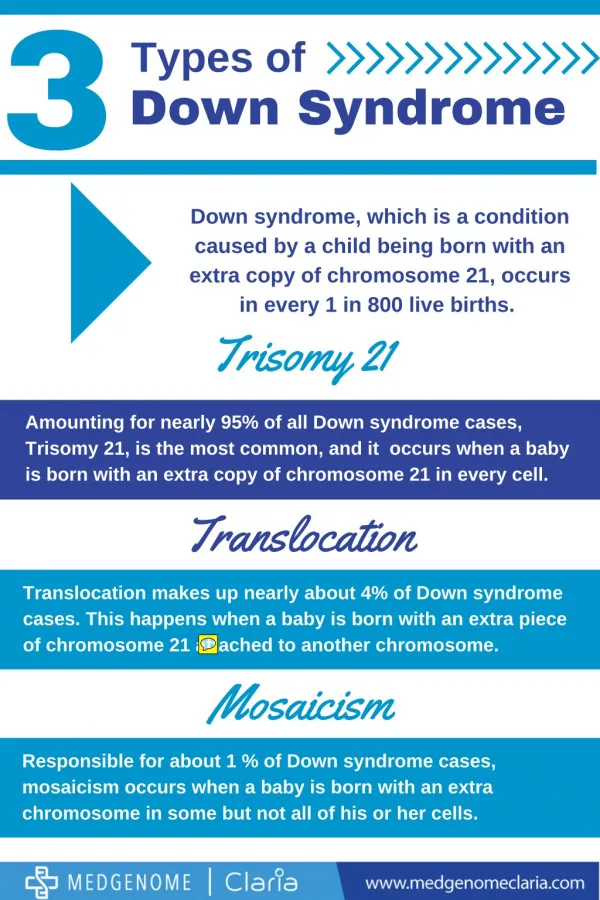
Prenatal (PN) Diagnosis • 1/300 pregnancies have recognizable chromosomal abnormalities • 95% are Trisomy 21, 18, 13, or changes in X and Y • Most of these are Down syndrome (DS) • Increasing maternal age increases risk of chromosomal abnormalities
Benefits of Prenatal Screening and Diagnosis • Parental reassurance (if normal) • Prenatal diagnosis may allow women to undertake a pregnancy they might not have otherwise undertaken • If abnormality detected: • Increased parental options • further testing • referral • counselling re planned birth or termination • preparation for special needs child • Altered obstetric management • Facilitated neonatal management
Risks of Prenatal Screening and Diagnosis • Parental anxiety • False positive • True positive • Pregnancy complications • Pregnancy loss
Prenatal Screening for Chromosome Abnormalities • Offer to all pregnant women • >90% of structural and chromosomal fetal abnormalities are born to low risk women • Maternal age alone poor screening tool • Only detects approx 30% of DS cases • 1996 CTFPHE recommended offering MSS to pregnant women
Prenatal Screening for Chromosome Abnormalities • Participation variable across Canada • Physicians routinely offering MSS to all pregnant women: • >85% Ontario family physicians • 85% Newfoundland family physicians • 22% Northern Alberta physicians • 48% uptake of MSS by pregnant women in Ontario What are concerns about MSS screening? • High false positive rate ~ 10% (7%DS, 3% NTD, 0.3% T18) Carroll et al CMAJ 1997, Chandra et al J Obstet Gynaecol Can 2003, McElligott et al ASHG Poster 2004, Summers et al J Med Screen 2003.
Options for Prenatal Screening for DS and trisomy 18 • Integrated Prenatal Screening (IPS) • Serum Integrated Prenatal Screening (Serum IPS) • First Trimester Screening (FTS) • Quadruple maternal serum screening (Quad) • Maternal serum screening (Triple) • Diagnostic tests: Amniocentesis/CVS What is available in your community?
Integrated Prenatal Screening (IPS) • 2 step screening combining: • T1 (11-13+ 6/7 weeks – ideally 11) • Nuchal translucency measurement • Maternal serum marker • PAPP-A (pregnancy-associated plasma protein) • T2 (15-20 weeks – ideally 15-17) • Maternal serum markers • AFP, uE3, hCG • Single risk assessment produced in second trimester
Nuchal Translucency • Subcutaneous fluid-filled space located between back of fetal neck and skin • Measured on U/S between 11–13+ 6/7 weeks, measurement is not valid outside of this time period • NT increases with gestational age • Between 11-13+ 6/7 weeks >3.0 or 3.5mm (depending on the centre) is considered elevated • Diagnostic testing indicated • Fetal echocardiogram indicated ~20 weeks (if NT>3mm) • Detailed anatomy scan at 18-20 weeks • Genetic counselling
Nuchal Translucency Increased NT associated with: • Trisomies 21, 18, 13, triploidy and Turner syndrome • Spontaneous fetal loss • With normal chromosomes: cardiac defects, diaphragmatic hernia, pulmonary defects, skeletal dysplasias, congenital infection, metabolic/haem disorders, rare single gene disorders • Normal pregnancy – chance of a normal birth varies with size of NT measurement Nicolaides. Am J Obstet Gynecol 2004;191:45 Souka et al.Ultrasound Onstet Gyncol 2001;18:9
Serum Integrated Prenatal Screening (SIPS) • Serum only - 2 step approach • Combines first and second trimester serum markers to produce single risk assessment • T1 • PAPP-A: 11-13+6/7 weeks • 11 weeks is ideal • T2 • AFP, uE3, hCG, Inhibin-A: 15–20 weeks • 15-17 weeks is ideal • Consider when NT not available False positive rate lower with a dating ultrasound
First Trimester Screening (FTS) • NT measurement: 11 to 13+6/7 weeks • T1 serum markers • PAPP-A, free beta hCG: 11-13+6/7 weeks • 11 weeks ideal • NTD screening with MS-AFP and/or ultrasound is still recommended in T2
Quadruple Screening • Second trimester maternal serum screening • 15-20 weeks – 15-17 weeks optimal • AFP, uE3, hCG, Inhibin-A Maternal Serum Screening (Triple) • Same as Quad screening but without Inhibin-A False positive rate lower with a dating ultrasound
Comparison of Prenatal Screening Tests Percent % PPV: 1 in 9 1 in 14 1 in 32 1 in 32 1 in 49 1 in 104
Prenatal Genetic Screening TestsOntario Data ** Summers AM et. al J Med Screen 2003 10:107-111. * Summers AM Personal communication
Diagnostic Testing • Chorionic Villus Sampling (CVS) • Performed at 10-14 weeks • Highly accurate for chromosome disorders • Early – first trimester • Not as widely available • Risk of fetal loss 1-2% • Higher rate of repeat procedures than amnio • Chance of ambiguous results
Diagnostic Testing • Amniocentesis • Performed from 15-20 weeks (15-17 ideal) • Results available 1-3 weeks later • Highly accurate • Risk of fetal loss 0.5-1%
What do women prefer? • Low false positive rate • High detection rate • Timing of results • Timing of termination
From the Literature… • A Dutch study of both high risk and low risk women found that both groups preferred FTS: • Women were given an information package about FTS, second trimester screening and diagnostic testing for DS. • 95% of high risk women preferred first trimester screening for Down syndrome to second trimester screening. • 80% of low risk women also preferred first trimester screening to second. DeGraaf IM et. al 2002 Prenat Diagn 22:624-629.
From the Literature… • A British study of 291 low risk women found that the majority of women preferred the IPS option to FTS: • The tests were presented in the following theoretical situation: • IPS results at 15 wks - 95%DR • 2% risk of miscarriage after diagnostic testing • FTS result at 12 wks - 80% DR • 3% risk of miscarriage after diagnostic testing Bishop AJ et. al 2004 BJOG 111: 775-779
The Basics of Counselling • Pre-test counselling • Gather information • Risk assessment • Patient education • Identify options – engage in dialogue • Promote autonomous decision-making • Psychological assessment • Non-directive
Patient Education • Available options • Difference between screening test and diagnostic test • Benefits and limitations of screening and diagnostic testing (if appropriate) • Option of no testing
Assist with Decision Making… • Explore values, experiences, beliefs • Family structure: other children, supportive partner, extended family, etc. • Encourage women to consider possibility of positive screen result in advance of test • Think about what they might do in response to result
…Assist with Decision Making • Encourage women to consider the possibility of a negative result • Relieve anxiety? • Is this information you want to know in advance? • Knowing in advance allows time to prepare for the birth of a special needs child, grieving for the loss of a healthy baby and time to adjust expectations.
Psychological Assessment • Consider: • Patient’s ability to deal with: • Uncertainty • Disability • Risk of miscarriage • Personal beliefs re option of termination • If wouldn’t consider termination – need to prepare for birth of affected child
Non-Directive • Offer informed choice • “No matter what their moral or religious beliefs” • Beliefs and behaviours may change in face of positive screen or amnio/CVS result • Consider: Your own beliefs and how they may… • Influence your counselling style • Differ from your patient’s beliefs Carroll et al. Can Fam Physician 2000; 46:614
Case 1 - Vanessa • Age 27 • 8 weeks pregnant • G2P1 • Previous pregnancy uncomplicated • Married for 5 years, healthy 3 year old daughter
Case 1 Vanessa …. • What prenatal genetic screening options would you discuss with Vanessa? • Discuss options with benefits, limitations, availability • New screening tests may require earlier first prenatal visit
Case 1 Vanessa …. • If Vanessa was 38…..? • Could go directly to CVS, amnio • FTS/IPS more accurate than age • What might affect her decision? • Miscarriage rate • Performance of amnio/CVS compared to IPS, FTS, MSS • May detect problems other than Down syndrome • Her perception of risk/morbidity associated with DS • Degree of certainty/uncertainty she can tolerate • Her personal/family/religious beliefs…
Case 2 - Marta • Age 34 • 17 weeks pregnant • To discuss result of IPS screen
Case 2 – Marta… • Results: COMMENTS AND RECOMMENDATIONS Down syndrome: The risk of Down syndrome is GREATER than the screening cut-off of 1 in 200 at term. If the gestational age is confirmed, counselling regarding the risks and benefits of AMNIOCENTESIS is suggested.
Case 2 – Marta… • How would you present the results?
Case 3 - Marie • 33 years old • G2P0 • Miscarriage last year • Trying to get pregnant for several years • 14 weeks pregnant • Following U/S for NT for IPS – you received report from radiologist indicating NT is elevated (4.0mm) for this gestational age • What would be important to discuss with Marie and her partner at this time?
Case 3 – Marie…. • Marie was referred for genetic counselling • Offered: • Complete IPS screening • Chromosome testing • Ultrasound 18 - 20 wks & echocardiogram 20 - 22 wks • Counselled re risk of miscarriage with CVS or amnio • May be even more significant for this couple in view of infertility and miscarriage
Pearls of prenatal genetic screening… Take a 3 generation family history • Look for: • Potential patterns of inheritance • Consanguinity • Family History of: • birth defects • mental handicap • stillbirths or childhood deaths • chromosome disorders • severe childhood conditions (MD, CF)
…Pearls of prenatal genetic screening Pregnancy History: • Maternal age ≥ 35 • 3 or more spontaneous abortions • Stillbirths • Childhood deaths • Infertility
…Pearls of prenatal genetic screening Consider carrier screening for: • Hemoglobinopathies – Mediterranean, African, Middle Eastern, Asian, Hispanic/South/Central American background • CBC → MCV <80 • Hemoglobin electrophoresis • Questions? – call genetics • To find a genetics centre near you: http://www.cagc-accg.ca/centre1.html
The “Ashkenazi” Panelprenatal screening • Ashkenazi Jewish refers to those individuals of Eastern European Jewish ancestry. • Patients may be referred to genetics for counselling and screening.